Pelvic Rehab Report
The official Herman & Wallace blog. New blogs post every Friday on topics relating to the field of pelvic floor dysfunction.
Our understanding of treating pelvic pain keeps growing as a profession. We have so many manual therapies such as visceral manipulation, strain counter strain, and positional release adding dimension to our treatment strategies for shortened and painful tissues. Pharmacologic interventions such as botox, valium, and antidepressants are becoming more popular and researched in the literature. We are beginning to work more collaboratively with vulvar dermatologists, urogynecologists, OB’s, family practitioners, urologists, and pain specialists.
 Pelvic rehab providers are in a unique position of being able to offer more time with each patient and to see our patients for several visits. Frequently we are the ones being told stories about how a particular condition is really affecting our patient’s life and the emotional struggles around that. We are often the one who gets a clear picture of our patient’s emotional and mental disposition. A rehab provider may realize that a patient seems to exhibit mental patterns in their treatment. It can be anxiety from how the condition is changing their life, difficulty relaxing into a treatment, poor or shallow breathing patterns, frequently telling themselves they will never get better, or being able to perceive their body only as a source of pain or suffering, losing the subtlety of the other sensations within the body. Yet, aside from contacting a physician, who may offer a medication with side effects, or referring to a counselor or psychologist, our options and training may be limited. Patients may be resistant to seeing a mental health counselor, and we have to be careful to stay in our scope.
Pelvic rehab providers are in a unique position of being able to offer more time with each patient and to see our patients for several visits. Frequently we are the ones being told stories about how a particular condition is really affecting our patient’s life and the emotional struggles around that. We are often the one who gets a clear picture of our patient’s emotional and mental disposition. A rehab provider may realize that a patient seems to exhibit mental patterns in their treatment. It can be anxiety from how the condition is changing their life, difficulty relaxing into a treatment, poor or shallow breathing patterns, frequently telling themselves they will never get better, or being able to perceive their body only as a source of pain or suffering, losing the subtlety of the other sensations within the body. Yet, aside from contacting a physician, who may offer a medication with side effects, or referring to a counselor or psychologist, our options and training may be limited. Patients may be resistant to seeing a mental health counselor, and we have to be careful to stay in our scope.
Research is showing us that meditation as an intervention can be very helpful in addressing these chronic pain issues.
In a study in the Journal of Reproductive Medicine, 22 women with chronic pelvic pain were enrolled in an 8 week mindfulness meditation course. Twelve out of 22 enrolled subjects completed the program and had significant improvement in daily maximum pain scores, physical function, mental health, and social function. The mindfulness scores improved significantly in all measures (p < 0.01).
The questions have arisen, if meditation alters opiod pathways, how can it be administered safely with prescription medications. However in a 2016 study in the journal of neuroscience, it was concluded that meditation-based pain relief does not require endogenous opioids.” Therefore, the treatment of chronic pain may be more effective with meditation due to a lack of cross-tolerance with opiate-based medications.” “The risks of chronic therapy are significant and may outweigh any potential benefits”, according the the journal of American Family Medicine. Meditation training can be a tool to help our patients manage their pain without risk of long term opiod use.
In the two day course, Meditation for Patients and Providers, participants will learn several different meditation and mindfulness techniques they can use for patients with different dispositions, and to tailor the most appropriate approach to specific patients. The aim of the course is to be able to work meditation into a treatment and a home program that is best suited for your patient. The course also covers self care, preventing provider burn out and ways to be more mentally quiet as a provider seeking to give optimal care with appropriate boundaries.
Fox, S. D., Flynn, E., & Allen, R. H. (2010). Mindfulness meditation for women with chronic pelvic pain: a pilot study. The Journal of reproductive medicine, 56(3-4), 158-162.
LEMBKE, A., HUMPHREYS, K., & NEWMARK, J. (2016). Weighing the Risks and Benefits of Chronic Opioid Therapy. American Family Physician,93(12).
Zeidan, F., Adler-Neal, A. L., Wells, R. E., Stagnaro, E., May, L. M., Eisenach, J. C., ... & Coghill, R. C. (2016). Mindfulness-Meditation-Based Pain Relief Is Not Mediated by Endogenous Opioids. The Journal of Neuroscience, 36(11), 3391-3397.
Urinary incontinence (UI) can be problematic for both men and women, however, is more prevalent in women. Incontinence can contribute to poor quality of life for multiple reasons including psychological distress from stigma, isolation, and failure to seek treatment. Patients enduring incontinence often have chronic fear of leakage in public and anxiety about their condition. There are two main types of urinary leakage, stress urinary incontinence (SUI) and urge urinary incontinence (UUI).

SUI is involuntary loss of urine with physical exertion such as coughing, sneezing, and laughing. UUI is a form of incontinence in which there is a sudden and strong need to urinate, and leakage occurs, commonly referred to as “overactive bladder”. Currently, SUI is treated effectively with physical therapy and/or surgery. Due to underlying etiology, UUI however, can be more difficult to treat than SUI. Often, physical therapy consisting of pelvic floor muscle training can help, however, women with UUI may require behavioral retraining and techniques to relax and suppress bladder urgency symptoms. Commonly, UUI is treated with medication. Unfortunately, medications can have multiple adverse effects and tend to have decreasing efficacy over time. Therefore, there is a need for additional modes of treatment for patients suffering from UUI other than mainstream medications.
An interesting article published in The Journal of Alternative and Complimentary Medicine reviews the potential benefits of yoga to improve the quality of life in women with UUI. The article details proposed concepts to support yoga as a biobehavioral approach for self-management and stress reduction for patients suffering with UUI. The article proposes that inflammation contributes to UUI symptoms and that yoga can help to reduce inflammation.
Surfacing evidence indicates that inflammation localized to the bladder, as well as low-grade systemic inflammation, can contribute to symptoms of UUI. Research shows that women with UUI have higher levels of serum C-reactive protein (a marker of inflammation), as well as increased levels of inflammatory biomarkers (such as interleukin-6). Additionally, when compared to asymptomatic women and women with urgency without incontinence, patients with UUI have low-grade systemic inflammation. It is hypothesized that the inflammation sensitizes bladder afferent nerves through recruitment of lower threshold and typically silent C fiber afferents (instead of normally recruited, higher threshold A-delta fibers, that respond to stretch of the bladder wall and mediate bladder fullness and normal micturition reflexes). Therefore, reducing activation threshold for bladder sensory afferents and a lower volume threshold for voiding, leading to the UUI.
How can yoga help?
Yoga can reduce levels of inflammatory mediators. According to the article, recent research has shown that yoga can reduce inflammatory biomarkers (such as interleukin -6) and C-reactive protein. Decreasing inflammatory mediators within the bladder may reduce sensitivity of C fiber afferents and restore a more normalized bladder sensory nerve threshold.
Studies suggest that women with UUI have an imbalance of their autonomic nervous system. The posture, breathing, and meditation completed with yoga practice may improve autonomic nervous system balance by reducing sympathetic activity (“fight or flight”) and increasing parasympathetic activity (“rest and digest”).
The discussed article highlights yoga as a logical, self-management treatment option for women with UUI symptoms. Yoga can help to manage inflammatory symptoms that directly contribute to UUI by reducing inflammation and restoring autonomic nervous system balance. Additionally, regular yoga practice can improve general well-being, breathing patterns, and positive thinking, which can reduce overall stress. Yoga provides general physical exercise that improves muscle tone, flexibility, and proprioception. Yoga can also help improve pelvic floor muscle coordination and strength which can be helpful for UUI. Yoga seems to provide many benefits that could be helpful for a patient with UUI.
In summary, UI remains a common medical problem, in particular, in women. While SUI is effectively treated with both conservative physical therapy and surgery, long-term prescribed medication remains the treatment modality of choice for UUI. However, increasing evidence, including that described in this article, suggests that alternative conservative approaches, such as yoga and exercise, may serve as a valuable adjunct to traditional medical therapy.
Tenfelde, S., & Janusek, L. W. (2014). Yoga: a biobehavioral approach to reduce symptom distress in women with urge urinary incontinence. The Journal of Alternative and Complementary Medicine, 20(10), 737-742.
A diagnosis of breast cancer means many different things to many different people. Regardless, receiving this diagnosis means some sort of treatment will likely follow. The types of treatment and outcomes are largely dependent on individual patient scenarios, however, one thing is for certain: A patient’s life will be forever changed after having received this diagnosis.
Historically, comprehensive care for a patient with breast cancer has focused on treatment and prevention. However, more and more women are surviving breast cancer every year. Therefore, more attention needs to be paid to survivorship. Once someone has survived cancer, comprehensive, quality care should obviously focus on preventing recurrence, however, it may also include guidance and counseling on maintaining a healthy lifestyle and addressing physical and psychosocial changes.
 A very recent 2016 article published in the Annals of Surgical Oncology discusses the subject of survivorship in breast cancer patients. This article suggests that the key to achieving successful outcomes for management of a breast cancer survivor is a multidisciplinary approach to help these survivors deal with the physical and psychosocial sequela resulting from their diagnosis.
A very recent 2016 article published in the Annals of Surgical Oncology discusses the subject of survivorship in breast cancer patients. This article suggests that the key to achieving successful outcomes for management of a breast cancer survivor is a multidisciplinary approach to help these survivors deal with the physical and psychosocial sequela resulting from their diagnosis.
As a pelvic rehabilitation provider, this is a very thought-provoking article as it outlines several areas in which I feel breast cancer survivors could benefit from physical therapy. A pelvic rehabilitation provider can be a valuable part of the multidisciplinary team that helps manage a breast cancer survivor towards positive and meaningful outcomes, ultimately enhancing their quality of life. The following are some areas addressed in the article in which a breast cancer survivor may need assistance to improve and support a meaningful quality of life.
Sexuality: According to this article, studies show treatment for breast cancer is associated with significant decrease in sexual interest, desire, arousal, and difficulty achieving orgasm and/or lack of sexual pleasure. Additionally, patients can also report pain with intercourse (dyspareunia) and/or vaginal dryness, which can lead to sexual dysfunction. Physical therapy can help by providing education on normal sexual response and lubricants, as well as help with tissue healing. Therapeutic techniques include exercise and manual treatments to areas that may be damaged from surgery, radiation, and chemotherapy. Additionally, exercise has been shown to improve self-image. Poor body image has been linked to sexual dysfunction following breast surgery (depending on the type “breast sparing techniques” versus mastectomy). This includes only some of the ways a physical therapist can help improve sexual dysfunction.
Lymphedema: According to the article, 30-70% of breast cancer patients experience lymphedema after treatment. Physical therapy can play an important role in the control and/or reduction of lymphedema. A physical therapist can provide helpful education, exercise, weight control, and, if needed, manual techniques and compression garments and bandaging.
Teachable moments after cancer diagnosis: A teachable moment is when you identify and seize an opportunity to educate your patient. After a life altering event or illness, people are more accepting of advice and change of lifestyle. As healthcare providers, we can utilize this time to help our patients improve outcomes by modifying their behavior. The cited article states there is clear evidence that physical activity decreases incidence and recurrence.There is additional evidence to show controlling weight and maintaining a normal body mass index (BMI) improves breast cancer survivor outcomes. A physical therapist can help a breast cancer survivor to develop a guided and progressive home exercise program to help them maintain normal BMI and participate in regular physical activity safely and regularly.
The discussed article, “Breast Cancer Survivorship: Why, What and When?”, sheds light on many areas of physical and psychosocial challenges that patients surviving breast cancer may deal with. This article also advocates that a multidisciplinary approach yields the greatest outcomes. I suggest that physical therapy can be a valuable part of the team when creating patient care plans for breast cancer survivors.
To learn more about breast cancer and outcomes based treatments, consider attending "Physical Therapy Treatment for the Breast Oncology Patient! The next course is taking place in Stockton, CA this September 24-25.
Gass, J., Dupree, B., Pruthi, S., Radford, D., Wapnir, I., Antoszewska, R., ... & Johnson, N. (2016). Breast Cancer Survivorship: Why, What and When?. Annals of Surgical Oncology, 1-6.
In the 16th century, a theory called Preformationism claimed that sperm contained a preformed, exceedingly minute body referred to as a homunculus, which eventually became a person. This idea of a tiny man had staying power, as today the homunculus is a “body map” based on how much of the cerebral cortex is devoted to sensing each part of the body. Although the idea of a 16th alchemist placing little bodies into a flask conjures a variety of tantalizing images, our program focuses on the mundane, contemporary version of the homunculus. So…what does this have to do with a course that addresses pelvic floor dysfunction? Everything.
 Emerging evidence indicates that therapies that include work to enhance body awareness/kinesthetic sense are potent and effective. Our professional training unfortunately, tends to over-emphasize a structural approach. The good news is that manual therapy, to some degree, enhances a client’s body awareness; but when we have more “tools” to capitalize on this synergy between manual therapy and improved body awareness, we have a potent “elixir” to promote change. To quote Deane Juhan, “touching hands are not like pharmaceuticals or scalpels…they are like flashlights in a darkened room.” By using the “flashlight”, we not only contribute to structural change, but neurological change – meaning the more we pay attention to a particular part of our body, the more “real estate” the brain devotes to that part of the body. Increasing the pelvic floor’s “footprint” on the brain can enhance function of the pelvic floor dramatically and quickly. Therefore, rehabilitation to address pelvic floor dysfunction benefits from weaving orthopedic, neurologic and mindfulness practices together.
Emerging evidence indicates that therapies that include work to enhance body awareness/kinesthetic sense are potent and effective. Our professional training unfortunately, tends to over-emphasize a structural approach. The good news is that manual therapy, to some degree, enhances a client’s body awareness; but when we have more “tools” to capitalize on this synergy between manual therapy and improved body awareness, we have a potent “elixir” to promote change. To quote Deane Juhan, “touching hands are not like pharmaceuticals or scalpels…they are like flashlights in a darkened room.” By using the “flashlight”, we not only contribute to structural change, but neurological change – meaning the more we pay attention to a particular part of our body, the more “real estate” the brain devotes to that part of the body. Increasing the pelvic floor’s “footprint” on the brain can enhance function of the pelvic floor dramatically and quickly. Therefore, rehabilitation to address pelvic floor dysfunction benefits from weaving orthopedic, neurologic and mindfulness practices together.
This program is designed to add a new dimension for the skilled pelvic floor practitioner and to also serve practitioners new to this area of practice. There is no internal manual work; rather we draw from our deep knowledge of Yoga, Tai Chi, along with other Chinese internal martial arts (that put lots of emphasis on the pelvic floor for performance) and Feldenkrais to address pelvic floor dysfunction. Some lessons focus directly on the pelvic region and others on integrating the pelvic floor with full body movement. Ultimately, our goal is to help you connect the dots between structural, functional movement and mindfulness practices, as this powerful triad offers practitioners a comprehensive, approach for treating pelvic floor dysfunction.
We hope you’ll come join in New York City on September 18th & 19th. If you do, wear comfortable clothes as the workshop is designed to provide participants opportunities to embody the work…emphasis is placed on labs more than lecture.
Don’t hesitate to contact us if you have any questions.
This email address is being protected from spambots. You need JavaScript enabled to view it.
This email address is being protected from spambots. You need JavaScript enabled to view it.
You wouldn't place a newborn in a crib without knowing the legs were firmly attached at the right angle to the base. You wouldn't jump on a hammock if the poles or trees were not firmly intact and upright to support the sling. Why would you treat a pregnant woman without checking if her hips were working optimally in proper alignment to support the pelvis, inside which a new life is developing? Let's hope higher level clinicians spend the extra effort to learn about the surrounding areas that affect our specialty, whether it is pelvic floor or spine or sports medicine.
 In 2015, Branco et al., published a study entitled, “Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum.” Eleven pregnant women voluntarily participated in this descriptive longitudinal study. Ground reaction forces (GRF), joint moments of force in the sagittal, frontal, and transverse planes, and joint power in those same 3 planes were measured and assessed during gait over the course of the first, second, and third trimesters as well as 6 months post-partum. The authors found pregnancy does influence the kinetic variables of all the lower extremity joints; however, the hip joint experiences the most notable changes. As pregnancy progressed, a decrease in the mechanical load was found, with a decrease in the GRF and sagittal plane joint moments and joint powers. The vertical GRF showed the peaks of braking propulsion decreases from late pregnancy to the postpartum period. A significant reduction of hip extensor activity during loading response was detected in the sagittal plane. Ultimately, throughout pregnancy, physical activity needs to be performed in order to develop or maintain stability of the body via the lower quarter, particularly the hips.
In 2015, Branco et al., published a study entitled, “Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum.” Eleven pregnant women voluntarily participated in this descriptive longitudinal study. Ground reaction forces (GRF), joint moments of force in the sagittal, frontal, and transverse planes, and joint power in those same 3 planes were measured and assessed during gait over the course of the first, second, and third trimesters as well as 6 months post-partum. The authors found pregnancy does influence the kinetic variables of all the lower extremity joints; however, the hip joint experiences the most notable changes. As pregnancy progressed, a decrease in the mechanical load was found, with a decrease in the GRF and sagittal plane joint moments and joint powers. The vertical GRF showed the peaks of braking propulsion decreases from late pregnancy to the postpartum period. A significant reduction of hip extensor activity during loading response was detected in the sagittal plane. Ultimately, throughout pregnancy, physical activity needs to be performed in order to develop or maintain stability of the body via the lower quarter, particularly the hips.
The same authors, in 2013, studied gait analysis in the second and third trimesters of pregnancy. Branco et al., performed a 3-dimensional gait analysis of 22 pregnant women and 12 non-pregnant women to discern kinetic differences in the groups. Nineteen dependent variables were measured, and no change was noted between 2nd and 3rd trimesters or the control group for walking speed, stride width, right-/left-step time, cycle time and time of support, or flight phases. Comparing the 2nd versus 3rd trimester, a decrease in stride and right-/left-step lengths decreased. The 2nd and 3rd trimesters both showed a significant decrease in right hip extension and adduction during the stance phase when compared to the control group. In this study, the authors also noted increased left knee flexion and decreased right ankle plantar flexion during gait from the 2nd to the 3rd trimester. The bottom line in this study, just as the more recent one suggests, pregnant women need a higher degree of lower quarter stability to ambulate efficiently throughout pregnancy.
Physical therapists are movement specialists with a unique opportunity to analyze how humans function, whether athletes or pregnant women (or even a pregnant athlete). How the hips move and whether or not proper muscles are firing can affect anyone’s gait. The extra demands on the pregnant body require more specific analysis of kinetics by therapists, thus directing the protocols for rehabilitation of this population. It should behoove every pelvic floor specialist, in particular, to attend a course like “Biomechanical Assessment of the Hip and Pelvis" or "Care of the Pregnant Patient" in order to provide patients with the optimal support for the natural “crib” women provide during pregnancy.
Branco, M., Santos-Rocha, R., Vieira, F., Aguiar, L., & Veloso, A. P. (2015). Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum. Scientifica, 2015, 580374. http://doi.org/10.1155/2015/580374
Branco, M., Santos-Rocha, R., Aguiar, L., Vieira, F., & Veloso, A. (2013). Kinematic Analysis of Gait in the Second and Third Trimesters of Pregnancy.Journal of Pregnancy, 2013, 718095. http://doi.org/10.1155/2013/718095
Posture is a concept that rehab clinicians have long hung our hats on, and yet updated models of evaluation and care take into account the truth that there are plenty of humans functioning in poor postures who do not complain of musculoskeletal pain or other dysfunctions. Is postural dysfunction always, or never, causative? As with many things in life, the answer is likely somewhere in between. If our patient arrives at the clinic with a dysfunctional posture and improving their alignment eases discomfort and improves function, we have provided help with addressing posture. It is also likely that we have spent a bit too much time lecturing on the elusive “ideal” posture, when in fact dynamic and adaptive postures are more often occurring throughout a person’s day. Certainly computer postures add to a patient’s movement challenge, and we continue to learn more about the best ways for patients to manage the otherwise potentially static and unhealthy positions that add to many of our patients’ issues.
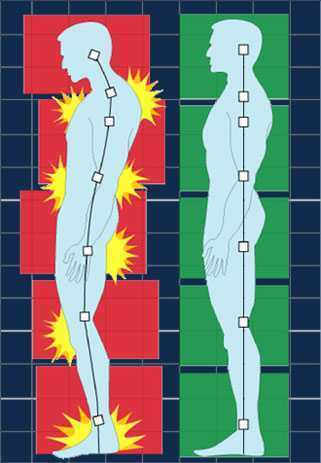 In regards to the pelvic floor, does changing standing lumbopelvic posture affect pelvic floor muscle (PFM) activation? This is the question asked by researchers from Queen’s University in Canada. (Capson et al., 2011) Sixteen women ages 22-41 who had never given birth and who were continent participated in the study. They were assessed completing five tasks in three different postures: normal lumbopelvic posture, hyperlordosis, and hypolordosis. The tasks included quiet standing, maximal effort cough, Valsalva maneuver, pelvic floor maximal voluntary contraction, and a load-catching activity. A vaginal sensor was to use to collect electromyographic activity of the pelvic floor, and sensors were placed on trunk muscles including the rectus abdominus, external and internal obliques, and erector spinae. A perineometer was utilized separately to record manometry measures, and 3D motion analysis was used to position women in the appropriate lumbopelvic angles. Key results of the investigation are summarized below:
In regards to the pelvic floor, does changing standing lumbopelvic posture affect pelvic floor muscle (PFM) activation? This is the question asked by researchers from Queen’s University in Canada. (Capson et al., 2011) Sixteen women ages 22-41 who had never given birth and who were continent participated in the study. They were assessed completing five tasks in three different postures: normal lumbopelvic posture, hyperlordosis, and hypolordosis. The tasks included quiet standing, maximal effort cough, Valsalva maneuver, pelvic floor maximal voluntary contraction, and a load-catching activity. A vaginal sensor was to use to collect electromyographic activity of the pelvic floor, and sensors were placed on trunk muscles including the rectus abdominus, external and internal obliques, and erector spinae. A perineometer was utilized separately to record manometry measures, and 3D motion analysis was used to position women in the appropriate lumbopelvic angles. Key results of the investigation are summarized below:
- Baseline EMG activity of the PFMs and the trunk muscles was significantly lower in supine versus standing
- PFM EMG activity in standing hypolordotic was higher than normal or typical posture
- Trunk muscle EMG activity did not significantly change during the 3 quiet standing postures
- For maximal PFM contraction and for cough, Valsalva, and load-catching, lower EMG activity was measured in standing in hyperlordotic or hypolordotic postures compared to “normal” or habitual posture
- With cough, all muscles except the erector muscles demonstrated increased activity
- In general, EMG activity was increased in trunk muscles when the subjects were in their habitual posture
- Related to timing of the rectus abdominus (RA) muscles, the RA were activated 106 ms before the PFM
- In standing, the intravaginal pressure was significantly higher in the hypolordotic posture compared to hyperlordotic posture
How can we put this valuable research to work in the clinic? This study validates a typical EMG activity finding of increased activity during standing versus lying, which makes sense given the pelvic tasks of working against gravity. In addition, it may be the case that our patients can generate an optimal amount of pelvic muscle contraction (when strengthening) in a more neutral posture. It may also be worth considering that for our patients who are chronically holding, perhaps a tendency for them to be in a hypolordotic posture is perpetuating their dysfunction. The data on timing of trunk and pelvic floor muscles was less consistent, although not less interesting. This research can also be implemented as an evaluation and intervention in the clinic- let’s be sure that we are using methods of feedback such as EMG, real-time ultrasound, or pressure biofeedback in various and functional positions. Then we can find out what seems to work best for our patient, whether the goal is to increase or decrease muscle activity and function.
Capson, A. C., Nashed, J., & Mclean, L. (2011). The role of lumbopelvic posture in pelvic floor muscle activation in continent women. Journal of Electromyography and Kinesiology21(1), 166-177.
Assuring patients with chronic pain they are not crazy by explaining the neurophysiology behind what is happening in their brain and body can be life changing. Increasing our patients’ knowledge about physical conditions can reduce anxiety and provide hope. As a healthcare provider, being confident in your differential diagnosis skills can help narrow down the physical source of pain, weed out the psychological components, and connect the dots to the neurological influence on the patient’s persistent symptoms.
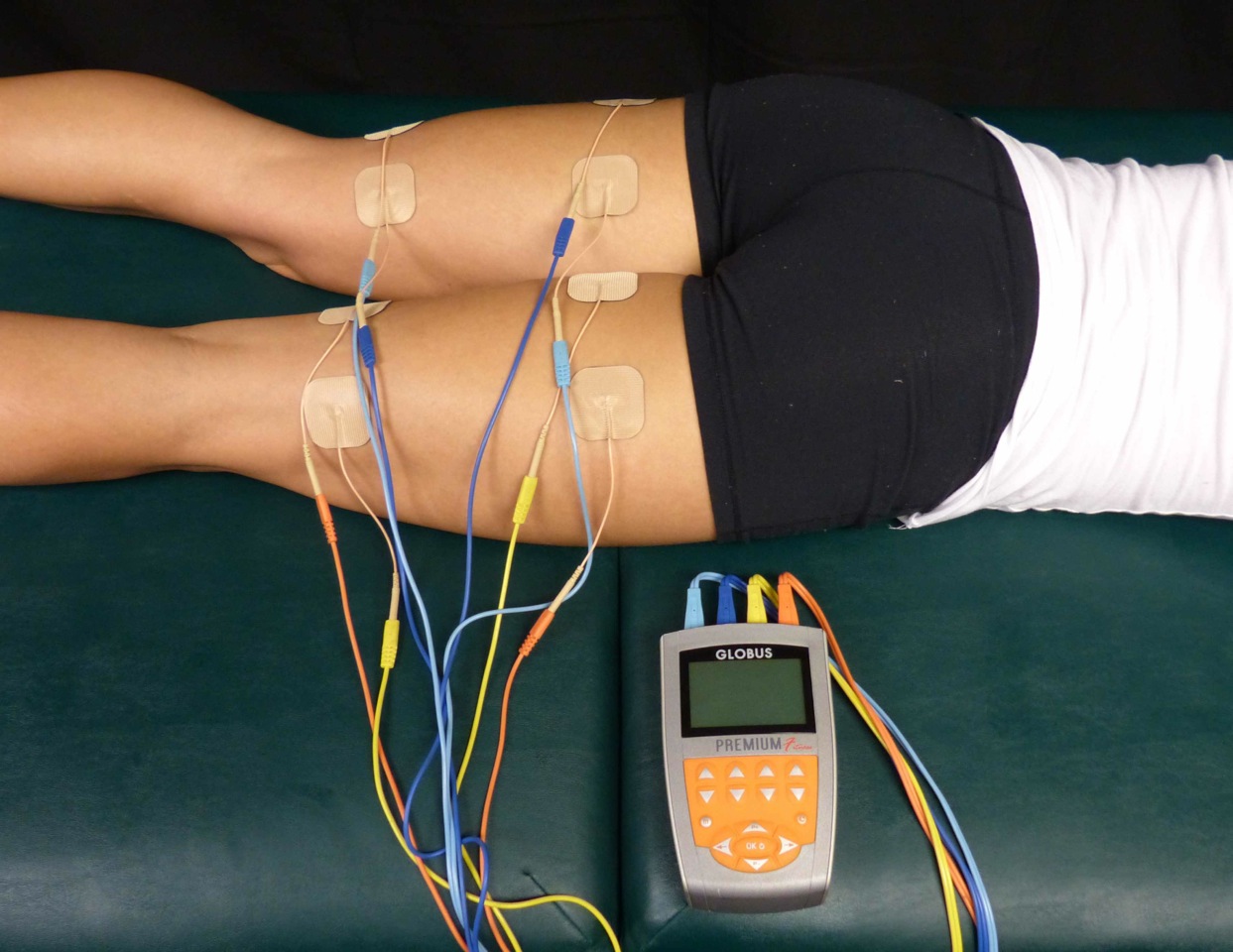 A 2015 article in Pain Medicine (Gurian et al) found a direct association between pain sensitivity and treatment of chronic pelvic pain. The study involved 58 women with at least 6 months of pelvic pain, and they were evaluated on pain threshold using transcutaneous electrical nerve stimulation before treatment and 6 months after a multidisciplinary approach to treatment of the pelvic pain. Pain intensity was also evaluated using the visual analog scale and the McGill questionnaire. Depending on the specific condition, treatment included manual therapy, physical therapy, pain medications, laparoscopy, oral contraceptives, nutrition intervention, or psychological support. After receiving treatment for 6 months, the pain threshold mean improved from 14.2 to 17.4. The effect sizes of 0.86 in the group with pain reduction and 0.53 in the group not achieving pain reduction were both within the 95% confidence interval. The authors concluded in this study that central sensitization does occur in patients with chronic pelvic pain, and treatment can reduce the general pain sensitivity of the patient.
A 2015 article in Pain Medicine (Gurian et al) found a direct association between pain sensitivity and treatment of chronic pelvic pain. The study involved 58 women with at least 6 months of pelvic pain, and they were evaluated on pain threshold using transcutaneous electrical nerve stimulation before treatment and 6 months after a multidisciplinary approach to treatment of the pelvic pain. Pain intensity was also evaluated using the visual analog scale and the McGill questionnaire. Depending on the specific condition, treatment included manual therapy, physical therapy, pain medications, laparoscopy, oral contraceptives, nutrition intervention, or psychological support. After receiving treatment for 6 months, the pain threshold mean improved from 14.2 to 17.4. The effect sizes of 0.86 in the group with pain reduction and 0.53 in the group not achieving pain reduction were both within the 95% confidence interval. The authors concluded in this study that central sensitization does occur in patients with chronic pelvic pain, and treatment can reduce the general pain sensitivity of the patient.
Kutch et al., (2015) performed a study regarding the change in men’s resting state of neuromotor connectivity as affected by chronic prostatitis or chronic pelvic pain syndrome (CP/CPPS), showing men are also subject to central sensitization. Fifty-five men (28 males with pelvic pain for at least 3 months and 27 healthy males) completed the study, with resting state functional magnetic resonance imaging detecting the functional connectivity of the pelvis with the motor cortex (pelvic-motor). The right posterior insula and pelvic-motor functional connectivity was found to be significantly different in men with chronic pelvic pain and prostatitis versus the healthy control group. Contraction of the pelvic floor corresponded with activation of the medial aspect of the motor cortex, while the left motor cortex was more associated with contraction of the right hand. The authors concluded this relationship may explain the viscerosensory and motor processing changes that occur in men with CP/CPPS and could be the most important marker of brain function alteration in this group of patients.
As more research is being done on the neurophysiological level of pain, more truth can support the “it’s all in your head” accusation. However, it is a positive light to shed for a patient. The brain is powerful and controls how pain is perceived globally. Proper treatment of a chronic pelvic floor condition, for women and men, can help reduce stress on the brain and lessen pain sensitivity and perception in our patients. Never let a patient pursue the self-perception that they are crazy. Explain central sensitization and how sometimes the brain wins in the war of “mind over matter”; however, give them hope, explaining how the proper treatment can lessen the intensity of the battle wounds.
Maria Beatriz Ferreira Gurian, Omero Benedicto Poli Neto, Julio Cesar Rosa e Silva, Antonio Alberto Nogueira, Francisco Jose Candido dos Reis. (2015). Reduction of Pain Sensitivity is Associated with the Response to Treatment in Women with Chronic Pelvic Pain. Pain Medicine. 16 (5) 849-854; DOI: 10.1111/pme.12625
Kutch, J. J., Yani, M. S., Asavasopon, S., Kirages, D. J., Rana, M., Cosand, L., … Mayer, E. A. (2015). Altered resting state neuromotor connectivity in men with chronic prostatitis/chronic pelvic pain syndrome: A MAPP: Research Network Neuroimaging Study. NeuroImage : Clinical, 8, 493–502. http://doi.org/10.1016/j.nicl.2015.05.013
III. Postpartum
Nourishing my baby and myself, a complicated dichotomy
 The care I received from the doctors, nurses, and hospital staff during labor, delivery, and postpartum period was excellent. I felt all the staff members explained all procedures for myself and the baby. The labor and delivery nurses were helpful and compassionate. They showed me how to breastfeed the baby, assisted me with skin to skin contact, and taught my husband and I how to care for the baby when we took her home. The birth center site at the hospital was amazing. I had an individual birthing suite with a bathroom, a television, a bathtub and a place for my husband to sleep. Health care for the baby and I following delivery continued to be excellent. I had a surgical follow up one week later with my doctor and another postpartum visit at 6 weeks. At each visit I was given The Edinburgh Postnatal Depression Scale (a scale to help identify postpartum depression) as well as educational pamphlets on self-care following a cesarean delivery. The only complaints I had that required assistance from a health care provider was with getting baby to latch with breast feeding and neck and shoulder pain from breast feeding the baby. I took it upon myself to work on core and hip exercises I would give a postpartum patient who had undergone a cesarean delivery and was working on my scar tissue to prevent problems with bladder, bowel, abdomen, and uterus. I sought some massage for my neck and shoulders and did my physical therapy exercises for my neck and shoulders. I sought a lactation consultant for the latching issues with breast feeding. Seeking care helped resolve these issues which reduced my neck and shoulder pain and helping me enjoy breastfeeding my baby.
The care I received from the doctors, nurses, and hospital staff during labor, delivery, and postpartum period was excellent. I felt all the staff members explained all procedures for myself and the baby. The labor and delivery nurses were helpful and compassionate. They showed me how to breastfeed the baby, assisted me with skin to skin contact, and taught my husband and I how to care for the baby when we took her home. The birth center site at the hospital was amazing. I had an individual birthing suite with a bathroom, a television, a bathtub and a place for my husband to sleep. Health care for the baby and I following delivery continued to be excellent. I had a surgical follow up one week later with my doctor and another postpartum visit at 6 weeks. At each visit I was given The Edinburgh Postnatal Depression Scale (a scale to help identify postpartum depression) as well as educational pamphlets on self-care following a cesarean delivery. The only complaints I had that required assistance from a health care provider was with getting baby to latch with breast feeding and neck and shoulder pain from breast feeding the baby. I took it upon myself to work on core and hip exercises I would give a postpartum patient who had undergone a cesarean delivery and was working on my scar tissue to prevent problems with bladder, bowel, abdomen, and uterus. I sought some massage for my neck and shoulders and did my physical therapy exercises for my neck and shoulders. I sought a lactation consultant for the latching issues with breast feeding. Seeking care helped resolve these issues which reduced my neck and shoulder pain and helping me enjoy breastfeeding my baby.
I have always felt that women in our country need better post-partum care and I am happy to see improvements being made
Before having my daughter, I had preconceived notions about postpartum care. For the last ten years since I started working with women’s health patients I have heard repeatedly from my patients that they felt they did not receive comprehensive postpartum care. Many of these women hopped from health care provider to health care provider, sometimes taking years to resolve orthopedic or pelvic floor problems from their pregnancy or labor and delivery experience. Quality postpartum care was my soap box issue and still is. That being said, I was very satisfied with my postpartum health care experience. My experience revealed that support and education about postpartum problems as well as proactive healthcare for theses challenges is becoming mainstream. I have always felt that women in our country need better post-partum care and I am happy to see improvements being made. We may forget between the constant baby changing, soothing, and feedings that mom needs some care too. I am not sure that we always remember that there have been 9 months of physiologic changes occurring to a woman’s body. Additionally, physical trauma that occurs with caesarean or vaginal delivery. A mother may need physical therapy for exercises to strength abdominals or back, help for bowel or bladder problems, manual therapy for painful intercourse, or scar tissue work for abdominals or pelvic floor.
I think as a society we are getting more aware of the influence of hormones, crying babies, sleep deprivation, and a heavy work load can overwhelm a postpartum mother. Based on my experience only, I think we are doing a better job of monitoring postpartum depression, pain management, and pelvic floor problems. I was so pleased at the availability of information and counseling opportunities presented to me during my birthing and postpartum experience. I received so much encouragement and permission to seek help from others during my postpartum healing.
Now that patients are being routinely counseled on postpartum self-care for mind and body we need to help them achieve successful outcomes. As health care providers, we should help postpartum patients decide how to include self-care with their new routine with baby. Caring for a baby takes a lot of time! My postpartum experience was likely similar to other women, where I had very little time to do all the “things I should be doing.” (For me this included neck, shoulder, abdominal, back, and pelvic exercises. As well as attending pediatrician, massage therapy, and lactation appointments.) The baby needs to feed constantly. By the time you feed, change, and soothe the baby (and pump if needed) it is almost time to do it again. You may never have more than an hour to get things done or get some sleep. As a mother there are many novel challenges to face, skills to learn, and emotional stress from fatigue and hormones. On top of all that, oh yeah, you should exercise, eat healthy, and if you are lucky shower and sleep! The point is, being a mother is challenging and we are all doing the best job we can. It is difficult to care for your baby while taking care of yourself. Reflecting back on my “birth story” has helped me empathize with my patients but also helped me to see that as health care providers, we should continue to provide education to our patients on self-care and continue to encourage them to seek care for their problems. However, to really help our patients successfully heal, we need to help them figure out how postpartum self-care blends into their new life with baby.
II. Labor and Delivery
The Baby Always Has a Different Plan
Towards the end of my pregnancy, my doctor ordered an ultrasound to make sure the baby was growing appropriately. This was precautionary as the baby had measured small the last couple appointments. The ultrasound gave us some important information. Baby K was growing appropriately, however, she was breech. At this point, she should have already flipped into the cephalic (head down) position, and it was unlikely that she would turn further along in my pregnancy. I knew what this meant… “C-section” (cesarean). Like so many women before me, this was not what I wanted for my birth plan. Having a planned cesarean had not really crossed my mind. I figured it would only be some kind of emergency that would result in this outcome. Instantly I thought of all the patients I have treated over the years who had cesarean delivery. I thought of abdominal adhesions and scar tissue mobility work that would need to be done postpartum. Naturally, as a physical therapist, I also thought of all the mobility challenges this would bring after baby. Having a cesarean would change my post-partum recovery; I would need more help with lifting, carrying, and we have so many stairs in our house! I know this may sound crazy… but what saddened me the most about cesarean delivery was that I was not going to experience what labor felt like. I felt cheated, in a weird way, I was looking forward to it, almost like a rite of passage. I wanted to analyze labor and delivery from a patient’s standpoint, not just as a therapist. I thought it would help me relate to patients and friends who have experienced labor. All that being said, a scheduled C-section was happening unless that baby miraculously flipped.
 My doctor suggested a version, which is a procedure where your doctor tries to manually turn your baby using an external technique. I had heard it is painful, but I pride myself on being a pretty tough woman who has dealt with some pain, I can do this! Needless to say, the version was painful… Very painful! As a matter of fact, the most painful procedure I have ever encountered. After trying about four times to turn the baby, my doctor asked me if we should try one more time. Although I was miserable, I asked if they thought the baby was close to being in the right position. The looks on my husband’s and doctor’s faces told me that she hadn’t moved at all. We gave it one more try, but that stubborn baby really liked the spot she was in. The plan was to proceed with the scheduled C-section at 39 weeks, unless I went into labor first, then it would be an emergency cesarean delivery.
My doctor suggested a version, which is a procedure where your doctor tries to manually turn your baby using an external technique. I had heard it is painful, but I pride myself on being a pretty tough woman who has dealt with some pain, I can do this! Needless to say, the version was painful… Very painful! As a matter of fact, the most painful procedure I have ever encountered. After trying about four times to turn the baby, my doctor asked me if we should try one more time. Although I was miserable, I asked if they thought the baby was close to being in the right position. The looks on my husband’s and doctor’s faces told me that she hadn’t moved at all. We gave it one more try, but that stubborn baby really liked the spot she was in. The plan was to proceed with the scheduled C-section at 39 weeks, unless I went into labor first, then it would be an emergency cesarean delivery.
At 39 weeks, I woke up the morning of the planned cesarean and thought, “it’s a good day to have a baby”. I was excited to finally meet this little princess, but a little nervous about the cesarean delivery. I was trying not to think about what was going to happen to my abdomen and uterus. I was hoping Baby K would handle all of this safely, and she would be well. My plan for the procedure was distraction, not to think about what was happening, as I knew too much. Sometimes ignorance is bliss. I did not want to think of every unfortunate story I had heard about “spinals”, and “cesareans gone wrong”, so I kept telling myself to trust my doctors and relax. After all, this is what they do every day, and they are good at it. I wasn’t the biggest fan of the numbness and tingling I felt in my legs, as well as the lack of motor control in the lower half of my body once they administered the spinal, but it did the trick.
All I felt during the caesarean was just some tugging on my abdomen as the doctor worked to get baby out and complete the procedure. Luckily, it was all happening behind a partition while my husband held my hand and we told jokes to relieve our nerves. All of a sudden, there was a loud cry, and I felt instant relief. It was my baby, and she had healthy lungs! My doctor popped around the screen and showed me my beautiful brown-haired baby. Next, my husband and the nurses cut the cord and took care of baby. Once she was cleared and safe, they plopped her on my chest. Like a moth to a flame, that baby wriggled herself right onto my breast. It was the purest form of instinct I have ever witnessed. How did that little baby that just entered this world have the innate knowledge to nourish, and the strength to find her food source. It was amazing! Overall, no matter how much you research and plan for labor and delivery, it likely won’t turn out how you plan it. The positive is that our bodies have been delivering babies forever, so trust in your body, and trust in those around you helping with the delivery. The labor and delivery experience is innate.
The following is the first in a three-part blog series which chronicles the peripartum journey of Rachel Kilgore.
I. Pregnancy
 In April, I had my first child, a sweet and healthy baby girl. Reflecting on the last year, what a ride! I have had many of my friends, family members, patients, and acquaintances discuss the journey and challenges of motherhood with me, however, experiencing it first hand was a memorable voyage. I thought I was very prepared and knew what I was getting into, but as usual, nothing compares to first-hand knowledge and experience. From an academic standpoint, I had done my research on everything from conception, what to expect each trimester of pregnancy, and reviewed the many options for labor and delivery. I even was lucky enough to assist in the Herman and Wallace Care for the Post-Partum Patient course with Holly Tanner while I was pregnant! As a practitioner, I love treating pregnant and post-partum patients, it is one of my favorite populations to treat. I love helping these strong, motivated women with pain relief and to teach them management skills to adapt to a new lifestyle and a changed body that has unique musculoskeletal needs.
In April, I had my first child, a sweet and healthy baby girl. Reflecting on the last year, what a ride! I have had many of my friends, family members, patients, and acquaintances discuss the journey and challenges of motherhood with me, however, experiencing it first hand was a memorable voyage. I thought I was very prepared and knew what I was getting into, but as usual, nothing compares to first-hand knowledge and experience. From an academic standpoint, I had done my research on everything from conception, what to expect each trimester of pregnancy, and reviewed the many options for labor and delivery. I even was lucky enough to assist in the Herman and Wallace Care for the Post-Partum Patient course with Holly Tanner while I was pregnant! As a practitioner, I love treating pregnant and post-partum patients, it is one of my favorite populations to treat. I love helping these strong, motivated women with pain relief and to teach them management skills to adapt to a new lifestyle and a changed body that has unique musculoskeletal needs.
First Trimester: Information, Nausea, and Fatigue
I had always had a preconceived notion that I would exercise diligently and eat super healthy through my pregnancy. After all, that was how my lifestyle was before pregnancy, why should it change? That lasted about 6 weeks, until 24-hour episodes of nausea and vomiting overwhelmed me, which continued until the start of the second trimester. I basically just tried to make it through the day without vomiting at work, and would go straight to bed whenever I had the chance. I even had to miss several days of work! I thought it was termed “morning sickness” implying that it went away after morning, but apparently it should be renamed to “forever nausea” as that is what it felt like at the time. Because of the nausea, I wanted nothing to do with food, which in turn lead to constant concern about the baby not getting enough nourishment. Of course, my regular activity levels plummeted. In addition to nausea was constant fear of miscarriage and whether my regular activities were somehow harmful to my baby. Instead of ice cream and pickles, I craved information. What should I be doing, and what should I not be doing?
Second Trimester: Return of Energy, Excitement, Planning and Doing!
When the first day of the second trimester hit, the nausea just went away. I was ecstatic! I got my energy back and was finally enjoying the pregnancy again! I was able to exercise regularly and eat healthy, two of my favorite things. Everything was going well, and it was time to start figuring out this whole baby thing. Luckily, most of my friends are mothers themselves, and they helped guide me. They directed me to great resources to satisfy my quest for knowledge about everything I needed to know for pregnancy, labor delivery, and the baby itself. They helped me decipher what all these baby products were, and what do you actually need. All the fun stuff was happening! We painted the baby’s room, ordered furniture, and planned a baby shower.
Third trimester: Waiting, Exhaustion, Heart Burn, and Reduced Mobility
Everything that happens to my patients happens to me. Third trimester was when I started to really “feel pregnant”. Daily mobility became challenging. I never realized how many times in a workday I show patients correct lifting mechanics or how often I set things on the ground or pick up weights. I started to dread every time I had to pick up something. At work, I would drop my pen on the ground so many times, and why had I never noticed that I did it so often? Luckily, I used my “physical therapy knowledge and skills” and did things I tell my pregnant patients to do; the results were minimal problems with musculoskeletal pain. Techniques such as: Using proper mechanics throughout my day, pulling in my core, and wearing a maternity support if my back was hurting a little. I never really developed severe back pain as is the case for many pregnant women. I completed hip and trunk exercises I usually give my pregnant patients and found they were easy to do and made me feel better... shocking right? Of course I was doing my kegels too! While my musculoskeletal system was doing well, my gastrointestinal system was not. I had never really had heart burn before, but now had it constantly, and found it to be very frustrating and depressing. I love cooking and eating but neither are enjoyable when you have heartburn. The heartburn was so bad it would wake me up every night coughing and chocking on my own acid reflux. Between lack of sleep, heartburn, and reduced mobility, I was getting pretty excited to be done with pregnancy and to finally meet “Baby K” as we had begun calling her. Overall, being pregnant was a very informative experience for me as a person and as a clinician. I often hear my patients tell me of their uncomfortable symptoms during pregnancy involving their musculoskeletal and gastrointestinal systems, however, now I empathize on another level.
By accepting you will be accessing a service provided by a third-party external to https://hermanwallace.com/
All Upcoming Continuing Education Courses

Rehabilitative Ultrasound Imaging: Pelvic Health Satellite Lab Course - Self-Hosted - April 19 - 21 2024 - SOLD OUT
Apr 19 2024 - Apr 21 2024
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024

Rehabilitative Ultrasound Imaging: Orthopedic Topics Satellite Lab Course - Cedar Knolls NJ - April 19 - 20 2024
Apr 19 2024 - Apr 20 2024
Rehabilitative Ultrasound Imaging: Pelvic Health Satellite Lab Course - Cedar Knolls NJ - April 19 - 21 2024
Apr 19 2024 - Apr 21 2024


Pelvic Function Level 2C - Satellite - Torrance CA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024



Pelvic Function Level 2C - Satellite - Springfield MO - April 20 - 21 2024
Apr 20 2024 - Apr 21 2024


Pelvic Function Level 1 - Satellite - New Bern NC - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024


Pelvic Function Level 1 - Satellite - Arlington VA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024


Pelvic Function Level 1 - Satellite - Omaha NE - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Bedford NH - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Leavenworth KS - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 1 - Satellite - Boston MA - April 20 - 21 2024 - SOLD OUT
Apr 20 2024 - Apr 21 2024

Pelvic Function Level 2B - Satellite - Seattle WA - April 27 - 28 2024 SOLD OUT
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Cranford NJ - April 27 - 28 2024 - SOLD OUT
Apr 27 2024 - Apr 28 2024

Menopause Transitions and Pelvic Rehab - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024


Pelvic Function Level 2B - Satellite - Des Plaines IL - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Hilton Head SC - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024












Pelvic Function Level 1 - Satellite - Kankakee IL - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024