
Rachel Kilgore, DPT, OCS, COMT, PRPC, PPCES graduated from Central Washington University with a Bachelor of Science (BS) in exercise science and a minor in nutrition in 2004 and completed her Doctor of Physical Therapy (DPT) at the University of Washington in 2007. Rachel practices in Seattle at Flow Rehab in the Freemont Neighborhood with Holly Tanner and focuses her patient care on orthopedics, female athletes, and women’s health conditions for bladder & bowel dysfunctions, pelvic, pain, pregnancy, and post-partum issues.
I have always been very particular about the precision of words. I have been known to ruminate about the origin, evolution, and application of words. As my husband always kindly says, I am an overthinker. This leads me to our nomenclature analysis for today, Diastasis.
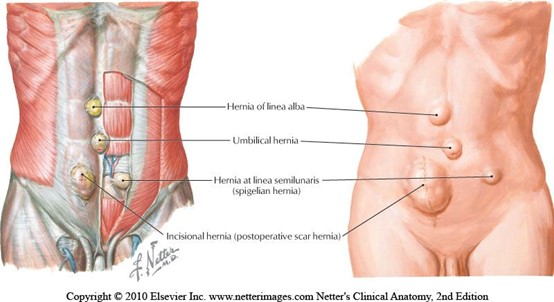 When teaching pregnancy and post-partum courses we always have healthy discussions about Diastasis Rectus Abdominus (DRA) as this is an important topic in the peripartum world. One question that always comes up is what is the difference between a hernia and DRA? If DRA is not a condition you deal with often in the clinic, it can be a bit confusing. According to the Merriam-Webster Dictionary diastasis means “an abnormal separation of parts normally joined together,” so DRA is often defined as a separation of the Rectus Abdominus muscles. I think the word separation is what causes the confusion. This word may lead some people to think there is an actual disruption of the abdominal tissue which is not the case. The rectus abdominus halves remain joined together by the linea alba. The linea alba is the tendinous raphe formed by interdigitating fascia of external/internal obliques and Transversus Abdominis. A DRA is an increase in the distance between the right and left Rectus Abdominus halves. If you stretch connective tissues (increase the distance between two ends), they may become thinner, lengthened, or weakened. A DRA is an increased distance between the right and left Rectus Abdominus halves that may result in lengthened, thinner, weaker tissue. In contrast, a hernia is an actual defect in the connective tissue. DRA and hernias are not the same thing; however, they can exist together.
When teaching pregnancy and post-partum courses we always have healthy discussions about Diastasis Rectus Abdominus (DRA) as this is an important topic in the peripartum world. One question that always comes up is what is the difference between a hernia and DRA? If DRA is not a condition you deal with often in the clinic, it can be a bit confusing. According to the Merriam-Webster Dictionary diastasis means “an abnormal separation of parts normally joined together,” so DRA is often defined as a separation of the Rectus Abdominus muscles. I think the word separation is what causes the confusion. This word may lead some people to think there is an actual disruption of the abdominal tissue which is not the case. The rectus abdominus halves remain joined together by the linea alba. The linea alba is the tendinous raphe formed by interdigitating fascia of external/internal obliques and Transversus Abdominis. A DRA is an increase in the distance between the right and left Rectus Abdominus halves. If you stretch connective tissues (increase the distance between two ends), they may become thinner, lengthened, or weakened. A DRA is an increased distance between the right and left Rectus Abdominus halves that may result in lengthened, thinner, weaker tissue. In contrast, a hernia is an actual defect in the connective tissue. DRA and hernias are not the same thing; however, they can exist together.
Let’s contrast these two conditions. Hernias can occur anywhere in the abdominal wall, whereas DRA is only at the midline. Hernia can strangulate intestines, but DRA does not as there is no hole or defect in the connective tissues. The only way to truly diagnose a hernia is by ultrasound. The only definitive treatment of a hernia involves surgery with closure of the hole, sometimes supported by mesh. Patients may elect to not have surgery if the hernia is small, is not painful, or if other conditions make surgery too risky. For diastasis, treatment rarely involves surgery. Hernias are disrupted fascia. Diastasis is lengthened, thinning, or weakened fascia.
 Diastasis Rectus Abdominus occurs commonly towards the end of pregnancy, with 66-100% of women having DRA by the end of the third trimester (Boissonnault & Blaschak, 1988; Mota et al, 2015). Mota et al. 2018 measured the distance between the two rectus halves in 84 primiparous women in the third trimester 2 cm below the umbilicus and found the average to be 49-79 mm. In contrast, a study of 150 nulliparous women (Beer et al.) showed the inter recti distance at that same point (2 cm below umbilicus) to be 16mm. However, DRA is not exclusive to the pregnant or postpartum person, they can exist in children and men as well.
Diastasis Rectus Abdominus occurs commonly towards the end of pregnancy, with 66-100% of women having DRA by the end of the third trimester (Boissonnault & Blaschak, 1988; Mota et al, 2015). Mota et al. 2018 measured the distance between the two rectus halves in 84 primiparous women in the third trimester 2 cm below the umbilicus and found the average to be 49-79 mm. In contrast, a study of 150 nulliparous women (Beer et al.) showed the inter recti distance at that same point (2 cm below umbilicus) to be 16mm. However, DRA is not exclusive to the pregnant or postpartum person, they can exist in children and men as well.
Another example of the word diastasis, where separation does not mean disruption, is with pubic symphysis diastasis. The words may be confusing. When a patient hears the word diastasis and is told it means separation, they may conclude they have a disrupted pubic joint. I think the definition of it from Stolarczyk et al. is much more descriptive and less likely to cause angst in a patient. “A pubic symphysis diastasis (PSD, diastasis symphysis pubis) is defined as excessive widening of the system of anatomical structures that make up the pubic symphysis (above the physiological norm of 10 mm), occurring during pregnancy or postpartum.”
This is another instance where the word separation may imply disruption when it just means increased distance.
Let’s return our thoughts to the title of this blog. I hope we are thinking about how the words we choose make our patients feel. Many of our patients receive a diagnosis and turn to the internet, where they may find confusing and even scary descriptions of their condition. If you were told that your abdominals had separated, doesn’t that sound scary? Would you feel nervous that your organs may fall out from your separated abdominals? I would have so many questions and fears! How will they get back together, what activities should I refrain from, can I even move? Wouldn’t the term separated make you feel scared to do anything? Think about the term separated shoulder, we hear it all the time in sports, we know it is a torn AC joint. There is an actual disruption of tissue, but DRA is not. As health care providers it is important that we use safe and encouraging words with our patients. Our role should be to educate them on their condition and make sure they understand the anatomy, physiology, and functional implications. We need to empower. The more a patient knows about their condition, the better choices they make regarding activity and lifestyle. Words are powerful.
References:
- Boissonnault, J. S., & Blaschak, M. J. (1988). Incidence of diastasis recti abdominis during the childbearing year. Physical Therapy, 68(7), 1082-1086.
- Mota, P., Pascoal, A. G., Carita, A. I., & Bø, K. (2018). Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskeletal Science and Practice, 35, 34-37.
- Beer, G. M., Schuster, A., Seifert, B., Manestar, M., Mihic‐Probst, D., & Weber, S. A. (2009). The normal width of the linea alba in nulliparous women. Clinical anatomy, 22(6), 706-711.
- Stolarczyk, A., Stępiński, P., Sasinowski, Ł., Czarnocki, T., Dębiński, M., & Maciąg, B. (2021). Peripartum Pubic Symphysis Diastasis—Practical Guidelines. Journal of clinical medicine, 10(11), 2443.

Kelly Sammis, PT, OCS, CLT, AFDN-S is a physical therapist, educator of dry needling and all things pelvic, Pilates instructor, wife, and mama living and working in Parker, Colorado. She specializes in the treatment of male and female pelvic floor dysfunction, athletic injury/return to sport, sports performance, and persistent pain. Her formal education took place at Ohio University (2007) and The University of St Augustine for Health Sciences (2010). Kelly serves as the lead faculty developing and teaching dry needling and pelvic health courses nationwide. Kelly co-instructs the Herman & Wallace Dry Needling courses along with fellow faculty member Tina Anderson, MS PT.
Pelvic floor dysfunction (PFD) is a common and relevant condition that affects many patients worldwide. According to our evidence, PFD can affect approximately 20-25% of women and men in the United States1, contributing to decreased participation in preferred daily, work and recreational activities due to high incidences of lumbopelvic pain, abdominopelvic pain, incontinence, prolapse, and/or other urologic and urogynecologic symptoms.2 These symptoms have a significant impact on a person’s quality of life and mental health status.2
While PFD is common, the general public has not been fully educated that these dysfunctions are not normal. As clinicians, we have a duty to educate our patient population that PFD is not a normal, nor acceptable, part of the postpartum experience or aging process. These dysfunctions are very debilitating but are also very treatable.
Common, not normal. Common, but treatable.
Pelvic floor pathology comes to us as clinicians in a variety of diagnoses, etiologies, and presentations2. Patients are often referred to physical therapy with medical diagnoses such as chronic pelvic pain syndrome (CPPS), interstitial cystitis, irritable bowel syndrome, endometriosis, dyspareunia, pudendal neuralgia, bowel and urinary incontinence, and chronic prostatitis.3-5 Symptom presentation is quite varied but often will include bowel, bladder, and sexual dysfunctions. That being said, a multidisciplinary approach is crucial to tailor treatment specific to each patient’s pathology, symptomatology, and clinical presentation.6 Many of these patients have seen a variety of gynecologists, urologists, and gastroenterologists without successful symptom mitigation and are being referred to pelvic health practitioners as a last resort. This is unfortunate, as a primary contributor to these symptoms is the neuromusculoskeletal system…and who better to treat the neuromusculoskeletal system than rehabilitative clinicians?!
Multimodal practice is key.
A well-rounded, multimodal treatment approach that is tailored to meet the patient’s specific goals is an important step in successfully treating PFD. Patient education can be a very powerful modality, which many clinicians tend to overlook. Research suggests education may help to address central nervous system upregulation and may help to retrain the brain in how it is processing input.7,8 While it is incredibly powerful to be able to influence pain processing, it doesn't stop with education. As clinicians, we also need to provide non-threatening, nourishing input to the tissues.
Manual therapies may help to desensitize the peripheral nervous system and surrounding soft tissues by providing neural input to alter the source of the pain and disruption.9,10 These techniques, including joint mobilization, soft tissue release, myofascial techniques, tool-assisted therapies, or any other manual approach, are likely addressing local tissue issues that may be perpetuating chronic pain or tissue dysfunction.
Dry needling is another effective and efficient technique that pelvic health practitioners can utilize to modulate the central nervous system, peripheral nervous systems and local tissues, including the pelvic floor directly.10 Dry needling encompasses the insertion of solid filament, non-injectate needles into, alongside or around muscles, nerves or connective tissues with or without mechanical and/or electrical stimulation for the management of pain and dysfunction in neuromusculoskeletal conditions.
While the detailed mechanisms of dry needling are not well known, we have seen more and more evidence that has provided us with an understanding on how to best utilize this technique in our clinical practice. Overall, it is thought that dry needling may address hypersensitive neural structures and spinal segments5, enhance treatment of myofascial pain and trigger points in the pelvic floor and surrounding musculature, and assist in the facilitation and/or inhibition of abnormal muscle tone and motor recruitment patterns.10-23 Dry needling has the ability to assist in addressing bladder, bowel, and sexual dysfunction alongside addressing pain syndromes in our patient population that is impacted by PFD.
Dry needling is one of the most effective tools we have as rehabilitative practitioners to reset dysfunctional tissue, providing effective and efficient functional changes for our patients. Ultimately, we are able to facilitate a more balanced resting tone, healthy motor recruitment patterns, and optimal neuromuscular utility to re-establish ideal function in our patients. The power of the tissue reset that dry needling provides has changed my clinical outcomes for the better and has also positively impacted and changed the lives of many of my clients. Want to add this tool to your clinical practice? Check out our course offerings with Herman & Wallace:
- Dry Needling and Pelvic Health - Waco, TX - June 11-12, 2022
Dry Needling and Pelvic Health - Milwaukee, WI - September 17-18, 2022
Dry Needling and Pelvic Health - Hatfield, PA - October 1-2, 2022
Dry Needling and Pelvic Health - Madison Heights, MI - October 8-9, 2022
Dry Needling and Pelvic Health - Worcester, MA - November 12-13, 2022 - Dry Needling and Pelvic Health: Advanced Concepts and Neuromodulation - Salt Lake City UT - November 5-6 2022
References:
- Hallock JK. The epidemiology of pelvic floor disorders and childbirth: an update. Obstet Gynecol Clin North Am. 2016 March;43(1):1-13
- Messelink et al. Standardization of Terminology of Pelvic Floor Muscle Function and Dysfunction: Report from the Pelvic Floor Clinical Assessment Group of the International Continence Society. Neurology and Urodynamics. 2005;24:374-380
- Anderson R, Sawyer T, Wise D, Morey A and Nathanson B. Painful Myofascial Trigger Points and Pain Sites in Men with Chronic Prostatitis/Chronic Pelvic Pain Syndrome. The Journal of Urology. 2009;182:2753-2758
- Hahn L. Chronic Pelvic Pain in Women. Lakartidningen. 2001;98:1780-5
- Kotarinos R. Myofascial Pelvic Pain. Curr Pain Headache Rep. 2012;16:433.438
- Srinivasan A, Kaye J, Moldwin R. Myofascial Dysfunction Associated with Chronic Pelvic Floor Pain: Management Strategies. Current Pain and Headache Reports. 2007;11:359-364
- Moseley G. Widespread Brain Activity During An Abdominal Task Markedly Reduced After Pain Physiology Eduction: fMRI Evaluation of a Single Patient with Chronic Low Back Pain. Australian Journal of Physiotherapy. 2005;51(1):49-52
- Moseley G. A Pain Neuromatrix Approach to Patients with Chronic Pain. Manual Therapy. Aug 2003;8(3):130-140
- Baron et al. Peripheral Input and Its Importance for Central Sensitization. Ann Neurol. 2013;74(5):630-6
- Chou L, Kao M, Lin J. Probably Mechanisms of Needling Therapies for Myofascial Pain Control. Evidence-Based Complimentary and Alternative Medicine. 2012;11
- Chen J, Chen S, Kuan T, et al. Phentolamine Effect on the Spontaneous Electrical Activity of Active Loci in a Myofascial Trigger Spot of Rabbit Skeletal Muscle. Archives of Physical Medicine and Rehabilitation. 1998;79(7):790-4
- Cummings T and White A. Needling Therapies in the Management of Myofascial Trigger Point Pain: A Systematic Review. Archives of Physical Medicine and Rehabilitation. 2001;82(7):986-992
- Gerber L, Shah J, Rosenberger W et al. Dry Needling Alters Triggers Points in the Upper Trapezius Muscle and Reduces Pain in Subjects with Chronic Myofascial Pain. Physical Medicine and Rehabilitation. 2015;7(7):711-718
- Gunn C, Milbrandt W, Little A et al. Dry Needling of Muscle Motor Points for Chronic Low Back Pain: A Randomized Clinical Trial with Long-Term Follow-Up. Spine. 1980;5(3):279-291
- Hsieh Y et al. Dry Needling to a Key Myofascial Trigger Point May Reduce Irritability of Satellite MTrPs. American Journal of Physical Medicine and Rehabilitation. 2007;86(5):397-403
- Lewit K. The Needle Effect in the Relief of Myofascial Pain. Pain. 1979;6(1):83-90
- Shah J. Uncovering the Biochemical Milieu of Myofascial Trigger Points Using In Vivo Microdialysis. Journal of Musculoskeletal Pain. 2008;16(1-2):17-20
- Shah J, Danoff J, Desai M et al. Biochemicals Associated with Pain and Inflammation are Elevated in Sites Near to and Remote from Active Myofascial Trigger Points. Archives of Physical Medicine and Rehabilitation. 2008;89(1):16-23
- Sterling M, Valentin S, Vicenzino B, et al. Dry Needling and Exercise for Chronic Whiplash - A Randomized Controlled Trial. BMC Musculskeletal Disorders. 2009;10:160
- Tough E, White A, Cummings T, et al. Acupuncture and Dry Needling in the Management of Myofascial Trigger Point Pain: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. European Journal of Pain. 2009;13(1):3-10
- Tuzun E, Gildir S, Angın E, et al. Effectiveness of Dry Needling Versus a Classical Physiotherapy Program in Patients with Chronic Low-Back Pain: A Single-Blind, Randomized, Controlled Trial. Journal of Physical Therapy Science. 2017;29(9):1502-1509
- Hong C and Torigoe Y. Electrophysiological Characteristics of Localized Twitch Responses in Responsive Taut Bands of Rabbit Skeletal Muscle Fibers. Journal of Musculoskeletal Pain. 1994;2(2):17-43
- Puentedura E, Buckingham S, Morton D, et al. Immediate Changes in Resting and Contracted Thickness of Transversus Abdominis After Dry Needling of Lumbar Multifidus in Healthy Participants: A Randomized Controlled Crossover Trial. Journal of Manipulative and Physiological Therapeutics. 2017;40(8):615-623


My name is Christina Trautman, and I am the Owner of The Pelvic Floor Place in Vancouver, WA. I am 39 years old and have been a practicing Pelvic Floor Physical Therapist for almost 14 years. I did not just stumble upon this career, it saved me.
I started having pelvic floor issues at the age of 7, peeing my pants when I would laugh. I had no physical trauma or incident as to why this was happening so as a 7-year-old, this was obviously humiliating and so embarrassing. This continued throughout elementary and went into middle school. When I was 13 and first got my period, I literally could not put in a tampon because my pelvic floor and vagina was so tight. This was frustrating and very inconvenient for an active sport-playing high schooler especially because all my friends could. What was wrong with me? I often felt alone and had no one I could talk to about my issues. After pleading with my mom to take me to a gynecologist for this difficulty and debilitating periods, I finally went as a sophomore in high school. It was the worst pain and experience of my life. Not only was I cramping for days and sobbing from the pain, but she told me, “You just need to have a kid and all your pain and issues will go away.”
Thankfully, I didn’t listen to her as getting pregnant at 14 wasn’t exactly the story I wanted and literally I probably couldn’t have sex if I tried. I continued to leak with laughing, couldn’t use a tampon, had debilitating periods, and was scared to death to date anyone. No one I knew had any of the same issues I had, and it wasn’t really a conversation my mom wanted to have with me. So, I continued to feel alone and in a lot of pain.
I compensated with my body throughout high school and college and couldn’t see improvement until I had Pelvic Floor Physical Therapy in my sophomore year in college. I was working as an aide in a PT clinic and luckily, they had a great Women’s Health PT there who noticed I had some pelvic floor symptoms. I was treated by her for a few years on and off and saw a huge improvement in my pain, leaking, and weakness. She connected the dots on all my issues that really stemmed from anxiety and an out-of-whack nervous system that started as a young kid after my parents divorced at the age of 3. After several treatments, I could put a tampon in, I didn’t leak with laughing, and was starting to get stronger in my core and pelvic floor.
I knew I had to go to PT school to treat women who had similar issues, so they too didn’t feel alone, embarrassed, humiliated, and frustrated.
My first job out of PT school was with that same therapist who treated me during college in Beaverton, OR. I took a Herman & Wallace Women’s Health class on a weekend before graduating from PT school and started studying all about the pelvic floor along with studying for my boards. She mentored me and I started seeing Women’s Health clients on day 1 of work. I loved it. This was my calling.
I split my time at that fast-paced office and a smaller clinic in Scappoose, OR. I was there for 2 years treating about 25-30% of women’s health clients. During that time, I took 3 different Herman & Wallace courses along with other classes dealing with Women’s Health. Every time I took a class, I wanted more. I wanted more complex clients and more time to treat them. I started dating a guy who lived in Vancouver WA, who is now my amazing husband, and I was ready for a change, so I took a job at a Chronic Pain clinic working as their Pelvic PT Specialist in Vancouver WA. I learned a ton and got to work with a good friend of mine. However, every day on my schedule, I would get so excited for my Pelvic clients and bored with my other orthopedic clients. So, I started looking for a full-time Pelvic PT position.
My best friend was working at a Pilates-based PT/Chiropractic office in Portland and they were looking for a Pelvic Floor PT. Despite the early morning hours and the long commute, I took the job. I was there for about 2 years and loved it. It was so fun working with chiropractors and skilled PTs. It was slow-paced but challenging and I was trained in Pilates Based PT. After getting pregnant, I decided the commute at 5 am to Portland was going to be too much so I took part-time jobs in Vancouver where I lived. This is when I opened my clinic.
I knew I always wanted to be a business owner; it was just so daunting. So, during my pregnancy, I slowly started seeing a couple of clients a week at my house while working part-time at other clinics in the area. This was amazing. I loved being in control of my own schedule and treating how I wanted to. I was mostly treating incontinence, prolapse, and pelvic pain but due to being pregnant, I started to get more interested in pregnancy and postpartum.
On December 25, 2017, I had my first baby, a 5-hour labor that I worked my tail off for. I had a great pregnancy and was highly active and ended up having a quick first vaginal birth with a very quick recovery. I owe that to all the exercises, breathing, and meditation I did during my pregnancy. I had a small tear with a natural vaginal birth but healed quickly with treatments I did on myself and was able to have sex within a few months with a supportive partner. Thinking about where I started to this point was miraculous. I did suffer from a grade 1 rectal prolapse about 5 weeks post-partum as I was struggling with constipation and a crying infant. As you can imagine, this was very frustrating as a Pelvic Floor PT, but those symptoms improved after I applied what I knew to my diet and exercises for my pelvic floor to help with strength and support. I owe all my success to having a supportive team to help me through my pelvic floor issues, pelvic floor PT, and a supportive partner. After recovering and getting back to work, I started taking more classes and getting certifications in pregnancy and postpartum classes. Ooh, this was my happy place. Starting to treat clients when the issues were really starting for most women was what I wanted to do.
I continued to slowly grow my business over the next few years as well as work at clinics in the area. It was a nice split. Enter my second pregnancy and covid. I had a great pregnancy and tried to keep as active as I could and the stress as low as I could. I had a 3-hour labor with no complications and a very fast recovery. How did I go from not being able to put a tampon in to delivering an 8 lb. baby without tearing? Pelvic PT is how! I truly was so proud and amazed at what my body could do. After I had Noah, I slowly started increasing my clientele and eventually decided to go full-time with my business.
During the last 5-6 years, I kept thinking about the Pelvic Rehab Practitioner Certification (PRPC) and kept putting it off for different reasons. After my son was about 2 and no longer requiring as much of my attention, I started studying for the test and passed in November of 2022. Woohoo!
I was still seeing clients at my house 4 days and week and in January of 2023 decided I needed to be in a real office. So, I joined forces with a prenatal chiropractor and a midwife group, and we opened up all 3 of our women-owned businesses in Felida, a small neighborhood and up-and-coming area near where I live. I am now mostly full-time, but I am as busy as I want to be while keeping a flexible schedule with the kids. I still have to work on my exercises and am aware of my pelvic floor, but I am no longer suffering with pain with sex, leaking, or weakness. I rewrote my story and yes while having kids did help (I will never tell that gynecologist that however), it really was Pelvic Floor Physical Therapy that has allowed me to live a normal life.
BIO:
Christina Trautman, PT, DPT, PRPC received her bachelor’s degree in Life Science from the University of Portland and her Doctorate in Physical Therapy from Pacific University. Through her personal experience with pelvic floor dysfunction and her extensive training, she found a passion for Women’s Health therapy and went on to take the Pelvic Floor Series courses (now Pelvic Function) through Herman & Wallace and holds her Pelvic Rehabilitation Practitioner Certification (PRPC).
Christina has been treating and aiding women with pelvic floor dysfunction for over 12 years and recently received her PRPC certification, making her one of the most sought-after pelvic floor rehab specialists in the area. She has also received her Postpartum Corrective Exercise Specialist Certification, Pre- and Post-Natal Corrective Exercise Specialist Certification, STOTT Rehab Pilates Mat and Reformer, and is pursuing more classes in pregnancy and postpartum care. She also treats orthopedic conditions and has a background in NAIOMT, ASTYM, and other manual therapy and exercise certifications.
Christina specializes in treating pregnancy and postpartum care, pain syndromes, pelvic organ prolapse, incontinence, and how to restore balance in the pelvic floor. She focuses on holistic care with a gentle approach to treating the pelvis and structures within the body that alter the mechanics of the pelvic floor. She also offers pregnancy and postpartum training programs.
Christina is the creator of The Pelvic Floor PlacePelvic Floor Place, and her desire is to treat women dealing with pelvic floor issues as well as helping pregnant and postpartum moms rehabilitate after having babies.
In her free time, she enjoys spending time with her family, getting outside, and enjoys working out with pilates, yoga, barre 3, and CrossFit.


It's been four years since my pelvic floor bestie (fellow Lead TA Carly Gossard) convinced my introverted self to try my hand at teaching assistant. I was hesitant, to say the least. I had taught small lab groups at Stockton University and mentored many of my colleagues in different areas, including pelvic health, but a class of 50 people relying on me to guide them through their first pelvic exam experience…I was terrified. It was the weekend before the world shut down for COVID, so there was this underlying current of “What does the future hold” and “Should we steal the gloves and hand sanitizer?”
Flash forward to the present day. I consider myself so lucky to wear many hats for Herman & Wallace. That first TA experience sparked this love of being with the Level 1 students as they embark on their pelvic health provider journeys. When HW needed to shift to the satellite model, I was one of the first TAs to jump into that role. When Megan Chamberlain (herder of the TAs) asked for help building a Lead TA program, I gave her my list of suggestions (I may consider Leslie Knope from Parks & Rec a role model). One of my favorite things about HW is that they take feedback seriously. At one point, they realized they needed someone to track the patterns of that feedback and guess who got that job….ME!
In 2023, the HW team decided it was time to take that feedback and update the main series to be more…more inclusive, more advanced, more hands-on, more to take home immediately to clinical practice. I was quick to chime in as I had a lot of subjective data from years of review synthesis. We have been organizing, researching, considering, consulting, and revamping the main series, and the first two classes of the series launched in January 2024! As the series rolled out, I decided I needed to TA each class to feel and experience the changes.
I spent January 14th and 15th at Hunter College in NYC with 30+ students during the second run of Pelvic Function Level 1. It went just as amazing as I had hoped as I helped the content team build it. The precourse work laid the foundation for more inclusive providers, reviewed the basics, and set students up to be ready for more advanced and hands-on content in class. There was penile-scrotal anatomy in this course instead of participants having to dive deeper into the pelvic floor series to learn these structures exist. It took about 2 years of my pelvic health career for that to happen in a class for ME! Students came in with more comfort on what they were going to do in person. They also confirmed that the workbook was the thing that hands-on, visual learners dream of. They even noticed we used bigger fonts and included closed captioning.
If you’ve interacted with me at all, through TA experiences, classes, or watching me mic run at HWConnect 2023, you’ll see I’ve come a long way from being the shy wallflower in the back of a PF1. This January, in addition to being one of the teaching assistants for Pelvic Function Level 1 in NYC, I’m also one of the first “TA Takeover” guinea pigs. What does this mean? Probably more videos of me dancing with pelvic organs from iHeartGuts joining the internet! I do hope to show you a little glimpse into what it's like to take a class with HW. In all seriousness though, HW’s goal and mission to bring quality, accessible, and inclusive care to all individuals makes it easy for me to say yes and sign up for any adventure they propose.

In this brief blog, I hope to explore several lifestyle medicine strategies (sleep hygiene, stress management, social connectedness) and how they may be included in therapeutic interventions to improve clinical outcomes. Frates and colleagues define lifestyle medicine as "The use of evidence-based lifestyle therapeutic approaches, such as a predominately whole-food and plant-based diet, regular physical activity, adequate sleep, stress management, avoidance of risky substance use, and other non-drug modalities to treat, oftentimes reverse, and prevent the lifestyle-related, chronic disease that's all too prevalent."1 Figure 1, adapted from the American College of Lifestyle Medicine, outlines the six pillars of lifestyle medicine.

Figure 1. Components of lifestyle medicine
Sleep Hygiene in Patient Education
The following are some simple patient education strategies that may help patients improve sleep:2-5
- Establish a regular bedtime and waking hours (avoid or minimize "social jet lag" that may be due to work, school, or your personal schedule).
- Create a comfortable room that is cool, dark, and quiet.
- Sleep in a comfortable bed and make sure it's not too old.
- Use a supportive and comfortable pillow and ensure it's not too old.
- Eliminate nighttime caffeine and limit daytime caffeine.
- Do not wear tight or restrictive clothing during sleep
- Avoid alcohol within 3 hours of bedtime.
- Do not smoke or use nicotine.
- Eliminate/limit after-dinner and late-night snacking.
- Limit or avoid computer use and smartphone use near bedtime.
- Avoid intense exercise near bedtime. However, do exercise and be physically active during the day.
- Maintain a healthy body mass index (BMI).
- Avoid watching intense television shows before bedtime.
- Turn off the radio and television before going to sleep.
- Avoid bright light near bedtime, but do increase daytime exposure to sunlight.
- Consider reducing your fluid intake near bedtime to avoid (or minimize) getting up to go to the bathroom, but maintain adequate hydration during the day.
- Minimize sugar and salt intake near bedtime as it may cause increased trips to the bathroom.
- Learn strategies to reduce daily stress so it does not result in poor quality and quantity of sleep.
- Minimize a tense or stressful lifestyle since this may carry over into sleep.
- Embrace mindfulness before bedtime
- Consider meditating close to bedtime or using a body scan or progressive muscle relaxation technique.
- Consider tai chi, qigong, or yoga later in the day.
- Establish a bedtime ritual such as:
- One hour before going to sleep, shut down all phone and computer devices. Then you can either read a book or watch a funny television show (drama may be too stimulating).
- Five minutes before you go to sleep, brush your teeth and floss, wash your hands and face with lavender soap, and shut off all the lights before slipping into your cozy bed with gratitude and pleasant thoughts.
Stress Management Patient Education
The following are some simple patient education strategies that may help patients manage stress:6
- Try yoga, tai chi, qigong
- Use aromatherapy (such as lavender)
- Engage in outdoor physical activities such as walking, hiking, and biking
- Engage in outdoor activities such as gardening
- Participate in hobbies such as reading, pottery, painting, and playing music
- Play with pets
- Get a massage
- Get involved in social activities such as volunteering, coaching, and community dancing
- Listen to music
- Smile and laugh more by watching comedy movies or television shows
Social Connectedness Patient Education
The following are some simple patient education strategies that may help patients improve socialization and social connectedness to form nurturing and constructive relationships:7-13
- Attend local sporting events, music performances, or art and museum exhibits.
- Connect with family and friends locally or on Zoom.
- Connect with your physician, therapist, wellness, or fitness professional via telehealth-delivered services.
- Create or join a community garden club.
- Create or join a lunchtime walking, yoga, or tai chi club.
- Engage in conventional group exercises such as softball, volleyball, basketball, pickleball, paddle tennis, or tennis.
- Engage in mind-body exercises such as yoga, tai chi, or Pilates.
- Engage in work-related community activities and fitness programs.
- Engage in small conversations with cashiers and employees at various stores you visit.
- Engage with members at your community place of worship.
- Enroll in art-based community activities, such as art, dance, drama, music, poetry, pottery, or expressive writing classes.
- Enroll at a local or community college to take cooking, history, or astronomy classes.
- Get a library card and participate in book club events.
- Get involved in nature-based activities, such as bird watching, botanical garden and park visits, farmer's market shopping, forest bathing or hiking, gardening, or walks at a lake, river, or beach.
- Join a group, such as a local bicycling club, chess, or table tennis club, or participate in your favorite hobby.
- Join a gym or fitness center.
- Join self-help groups.
- Join social media platforms like LinkedIn, Facebook, Twitter, Instagram, or TikTok.
- Play with your pets.
- Volunteer at a community center, hospital, school, or library.
- Volunteer to coach sports or mentor students.
- Walk with a mall club or create one in your neighborhood
If you are interested in learning more about these topics and others, please see my course Integrative and Lifestyle Medicine Toolbox for Rehab and Pain Management with Herman & Wallace.
Resources for Clinicians:
Learn how to include integrative and lifestyle medicine into your clinical practice with these resources:
- Academy of Integrative Health & Medicine
- American College of Lifestyle Medicine
- American College of Preventive Medicine
- Institute of Lifestyle Medicine
- National Center for Complementary and Integrative Health
Instructor Bio:
 Ziya "Z" Altug, PT, DPT, MS, OCS is a board-certified doctor of physical therapy with 32 years of clinical experience treating musculoskeletal injuries. Z currently provides outpatient physical therapy in the home setting in Los Angeles, California, and serves as a continuing education instructor.
Ziya "Z" Altug, PT, DPT, MS, OCS is a board-certified doctor of physical therapy with 32 years of clinical experience treating musculoskeletal injuries. Z currently provides outpatient physical therapy in the home setting in Los Angeles, California, and serves as a continuing education instructor.
Z received his Bachelor of Science in Physical Therapy at the University of Pittsburgh in 1989, Master of Science in Sport and Exercise Studies in 1985 and Bachelor of Science in Physical Education in 1983 from West Virginia University, and a Doctor of Physical Therapy from the College of St. Scholastica in 2015. Z is a long-standing member of the American Physical Therapy Association and a member of the American College of Lifestyle Medicine. He has attended workshops in yoga, tai chi, qigong, Pilates, Feldenkrais Method, and the Alexander Technique.
Z is the author of the books Integrative Healing: Developing Wellness in the Mind and Body (2018), The Anti-Aging Fitness Prescription (2006), and Manual of Clinical Exercise Testing, Prescription, and Rehabilitation (1993). In 2020, he published the chapter Exercise, Dance, Tai Chi, Pilates, and Alexander Technique in The Handbook of Wellness Medicine. In 2021, he published the article Lifestyle Medicine for Chronic Lower Back Pain: An Evidence-Based Approach in the American Journal of Lifestyle Medicine.
References:
- Frates, B., Bonnet, J.P., Joseph, R., & Peterson, J.A. (2019). Lifestyle Medicine Handbook: An Introduction to the Power of Healthy Habits. Monterey, CA: Healthy Learning.
- Altug Z. Integrative Healing: Developing Wellness in the Mind and Body. Springville, UT: Cedar Fort, Inc.; 2018.
- Kryger MH, Roth T, Goldstein CA. Principles and Practice of Sleep Medicine (2 Volume set), 7th ed. Philadelphia, PA: Elsevier; 2021
- Matsuo T, Miyata Y, Sakai H. Effect of salt intake reduction on nocturia in patients with excessive salt intake. Neurourol Urodyn. 2019;38(3):927-933.
- Vitale KC, Owens R, Hopkins SR, Malhotra A. Sleep hygiene for optimizing recovery in athletes: review and recommendations. Int J Sports Med. 2019;40(8):535-543.
- American College of Lifestyle Medicine. Handout: Lifestyle stress reduction. American College of Lifestyle Medicine; 2019.
- Leavell MA, Leiferman JA, Gascon M, Braddick F, Gonzalez JC, Litt JS. Nature-based social prescribing in urban settings to improve social connectedness and mental well-being: a review. Curr Environ Health Rep. 2019;6(4):297-308.
- National Institutes of Health. Social Wellness Toolkit. Bethesda, MD: National Institutes of Health. Accessed on June 2022.
- Roland M, Everington S, Marshall M. Social prescribing - transforming the relationship between physicians and their patients. N Engl J Med. 2020;383(2):97-99.
- Choi NG, Pepin R, Marti CN, Stevens CJ, Bruce ML. Improving social connectedness for homebound older adults: randomized controlled trial of tele-delivered behavioral activation versus tele-delivered friendly visits. Am J Geriatr Psychiatry. 2020;28(7):698-708.
- Davidson KW, Krist AH, Tseng CW, et al. Incorporation of social risk in US Preventive Services Task Force recommendations and identification of key challenges for primary care. JAMA. 2021;326(14):1410-1415.
- Eder M, Henninger M, Durbin S, et al. Screening and interventions for social risk factors: technical brief to support the US Preventive Services Task Force. JAMA. 2021;326(14):1416-1428.
- Steinman L, Parrish A, Mayotte C, et al. Increasing social connectedness for underserved older adults living with depression: a pre-post evaluation of PEARLS. Am J Geriatr Psychiatry. 2021;29(8):828-842.
Integrative and Lifestyle Medicine Toolbox for Rehab and Pain Management

Course Dates:
January 21, 2023
Price: $125
Experience Level: Beginner
Contact Hours: 4.5
Description: This course was written and developed by Ziya “Z” Altug, PT, DPT, MS, OCS, a board-certified doctor of physical therapy with 32 years of experience in treating musculoskeletal conditions, Brief lectures on the research and resources and labs will cover a toolbox approach for creating clinically relevant pain, anxiety, depression, and stress management strategies using lifestyle medicine, integrative medicine, expressive and art-based therapies, and the impact of nature on health. Participants will be able to practice Tai Chi/Qigong, expressive and art-based therapies including Music, Dance, and Drama Therapy, nature and aromatic therapies, self-hypnosis, and self-massage.

Kristina Koch, PT, DPT, is a board-certified clinical specialist in women’s health physical therapy and a certified lymphedema therapist. Kristina has been treating pelvic health conditions in individuals of all ages and genders since 2001 and works in private practice in Colorado Springs, CO. She has served as a guest lecturer for the pelvic health curriculum at Regis University in Denver and for the 3rd year medical students at the University of Colorado, Colorado Springs campus. She is the creator of Pharmacologic Considerations for the Pelvic Health Provider.
Although it is not within the scope of practice for rehab therapists to manage medications, it’s important that we review patient medications during the initial evaluation and on an ongoing basis. Therapists have a duty to assess medications impact on treatment and patient outcomes and to ensure patient safety. The population is aging and many patients over the age of 65 are on more than 5 medications, increasing the risk of medication side effects, adverse drug reactions, and drug interactions.
Primary care providers spend approximately 14-17 minutes with a patient during a visit, and the patient gets about 5 minutes to discuss their concerns, leaving little time for medication reconciliation or discussion regarding medication side effects (Tai-Seale, McGuire & Zhang, 2007). As therapists, we tend to see our patients for longer periods of time and more frequently, giving the patient more of an opportunity to discuss their signs and symptoms. Additionally, patients referred for pelvic health issues are often seeing multiple specialty providers (Ob/Gyn, urology, urogynecology, pain management, etc.) for their care, and each one is typically prescribing medications, potentially leading to polypharmacy. Understanding a medication’s actions, its impact on therapy, the side effects, and potential adverse drug reactions, can help guide treatment and improve patient outcomes.
A recent patient example is a post-menopausal cisgender female, referred by her primary care physician, for urinary urgency and nocturia. Her past medical history was significant for breast cancer. Her medications included an aromatase inhibitor, antihistamine due to seasonal allergies, and Vitamin C. After reviewing her medications and history, I recommended a non-hormonal vaginal lubricant and within 2 weeks her symptoms were 80% improved. Understanding the side effects of her medications allowed me to educate the patient about the effects of her medication and how to manage her symptoms.
More and more patients are attending therapy through direct access. As the first point of contact for patients, it's imperative that rehab professionals have a foundational knowledge of the medications often prescribed to treat pelvic floor conditions, GI, GU, and reproductive health issues. The ability to have educated conversations with our patients and other healthcare providers involved in their care can greatly improve the quality of care and outcomes, and maintain patient safety. The ability to discuss medications, vitamins, and supplements or complementary alternatives, that can minimize side effects, have fewer impacts on quality of life, and enhance function is an integral part of comprehensive patient care.
Join Kristina on Saturday, January 7, 2023, for Pharmacologic Considerations for the Pelvic Health Provider. This one-day, remote course will discuss the importance of understanding pharmacology and medication review, the current research regarding the pharmacologic treatment of numerous pelvic and reproductive health conditions and their side effects, drug interactions, and non-pharmacologic alternatives that are available for pelvic and reproductive health. Registration information and additional details are available at www.hermanwallace.com. #hermanwallacepelvicrehab, @hermanwallacepelvicrehab
References:
Ciccone, C. D. (2007). Pharmacology in Rehabilitation. (4th ed.). F.A. Davis Company.
Tai-Seale, M., McGuire, T.G., & Zhang, W. (2007). Time allocation in primary care office visits. Health Services Research. 42(5), 1871-1894. Doi: 10.1111/j.175-6773.2006.00689.x
Janes, M., & Kornetti, D. (2017). Medications: defining the role and responsibility of physical therapy practice. https://www.fsbpt.org/Portals/0/documents/free-resources/WinterForum2017Medications.pdf?ver=pf8bn4ZwoorAAg1PECZLfw%3D%3D
Pharmacologic Considerations for the Pelvic Health Provider

Course Dates:
January 7, 2023
Price: $200
Experience Level: Beginner
Contact Hours: 7.5
Description: This seven-and-a-half hour, one-day remote learning course will discuss medications used for the treatment of pelvic floor and genitourinary conditions as well as common side effects of medications routinely used for pelvic floor dysfunction. This course will be taught by Kristina Koch, PT, DPT via Zoom. Medications for constipation and GI dysfunction, as well as pelvic pain conditions such as Vulvodynia, Chronic Prostatitis, and Endometriosis, will be covered. The course will also cover medications and side effects in Gender-Affirming Care for patients who are transitioning.

Allison Ariail, PT, DPT, CLT-LAANA, BCB-PMD is one of the creators of the Herman & Wallace Oncology of the Pelvic Floor Course Series. Allison Ariail is a physical therapist who started working in oncology in 2007 when she became certified as a lymphatic therapist. She worked with breast cancer, lymphedema patients, head and neck cancer patients, and the overall oncology team to work with the whole patient to help them get better. When writing these courses, Allison was part of a knowledgeable team that included Amy Sides and Nicole Dugan among others.
As pelvic rehab professionals, we know the importance of the microbiome of the digestive tract and how this can influence issues our bowel patients may experience. You also may know that the GI microbiome can influence immune function as well as mental health. Did you know that the urinary bladder has its own microbiome? Recent developments in next-generation sequencing and bioinformatic platforms have allowed for the detection of microbial DNA in the urinary tract.(1) This could be a game changer for those who suffer from chronic urinary tract infections. However, it could be even more important as a way to prevent bladder cancer. May is Bladder Cancer Awareness Month. In honor of this month, let’s further discuss how the urinary microbiome may influence the development of bladder cancer.
Dysbiosis of the urinary microbiome could be related to bladder cancer through chronic inflammation in the urothelial microenvironment. Chronic inflammation is a hallmark of genomic instability and the development of cancer. A study in 2021 compared the urinary microbiome of patients with muscle-invasive and non-muscle-invasive bladder cancer. They found the microbial profiles differed in patients with cancer compared to healthy individuals. They also found that there were different microbial profiles from the less invasive non-muscle invasive versus the more invasive types of bladder cancer.(2)
The urinary microbiome is a growing area of research and I would expect to see more information come out on this, what influences the urinary microbiome, as well as how modulating this can prevent and fight urothelial cell carcinoma. I would anticipate more treatment options including some new immunotherapy agents to emerge that can help to fight bladder cancer.
If you do not know much about bladder cancer and would like to learn more, Oncology of the Pelvic Floor Level 2B covers topics on bladder cancer and gynecological cancers. Join us to learn more about these diagnoses, medical treatments, and ways a pelvic rehab professional can help these patients recover.
Resources:
1. Neugent ML, Hulyalkar NV, Nguyen VH, Zimmern PE, and De Nisco NJ. Advances in understanding the human urinary microbiome and its potential role in urinary tract infection. mBio. 2020; 11(2): e00218-20.
2. Hussein AA, Elsayed AS, Durrani M, et al. Investigating the association between the urinary microbiome and bladder cancer: an exploratory study. Urol Oncol. 2021; 39(6): 370.e9-370e19.

*Certified Lymphatic Therapists may skip Oncology of the Pelvic Floor Level 1 and move on to the Level 2A and Level 2B courses.*
Oncology of the Pelvic Floor Level 1 - no partner needed for registration
Price: $550.00 Experience Level: Beginner Contact Hours: 17.5 hours
Description: The course will address issues that are commonly seen in a patient who has been diagnosed with cancer such as cardiotoxicity, peripheral neuropathy, and radiation fibrosis. Some holistic medicine topics, including yoga and mindfulness, will be discussed in order to fully prepare the participant to be able to competently work with cancer survivors.
The basics of the lymphatic system will be covered, as well as when to refer the patient to a lymphatic specialist for further treatment. Red flags and warning symptoms will be discussed so the participant feels comfortable with knowing when to refer the patient back to their medical provider for further assessment.
This introductory course is aimed to get the participant comfortable with working with oncology patients and as part of an interdisciplinary oncology team.
Course Dates: July 8-9 and December 2-3
Oncology of the Pelvic Floor Level 2B - partner needed for registration
Price: $600.00 Experience Level: Intermediate Contact Hours: 19.25 hours
This course was designed to build on the information that was presented in Oncology of the Pelvic Floor Level 1.
Description: Information will be provided focusing on gynecological and bladder cancers including risk factors, diagnosis, and prognosis. The participant will also understand the sequelae of the medical treatment of cancer and how this can impact a patient’s body and quality of life. Other topics include rehabilitation and nutritional aspects focusing on these specific cancers, as well as home program options that patients can implement as an adjunct to therapy.
Course Dates: December 9-10

Megan Pribyl, PT, CMPT is a physical therapist at the Olathe Medical Center in Olathe, KS treating a diverse outpatient population in orthopedics including pelvic rehabilitation. Megan’s longstanding passion for both nutritional sciences and manual therapy has culminated in the creation of her remote course, Nutrition Perspectives for the Pelvic Rehab Therapist, designed to propel understanding of human physiology as it relates to pelvic conditions, pain, healing, and therapeutic response.
I have always viewed resultant health as the sum total of nutrition, exercise, lifestyle factors, environmental/toxicant & chemical exposure, genetics, and spiritual confluences. In balance, health and vitality flourish. Out of balance, health struggles manifest. If we take a look around, we bear witness to modern culture’s harmful effects upon our physiology – and specifically on our blood-brain barrier (BBB). Health struggles affecting the brain and impacted by BBB dysfunction are diverse and can include anxiety, depression, chronic pain, and neurodevelopmental disorders. Other disorders linked to a compromised BBB include Alzheimer’s disease, dementia, Parkinson’s Disease, and MS. So we ought to care a lot about our BBB – yet most of us don’t make conscious lifestyle choices based on protecting this vital gatekeeping system. Perhaps if we examine one specific angle of this issue - that diet and short-chain fatty acids influence the integrity of the blood-brain barrier – we might decide to care a lot more about protecting our brain – like we mean it.
For starters, it helps to acknowledge that our entire body IS an immune system – one that is constantly surveying potential threats to our existence. It is very well established that 70% of our immune system resides in our gut. This placement makes sense because the very act of eating exposes our inner workings to whatever “food” passes through the alimentary canal. Our digestive tract is a frontline sorting station that decides what can pass through the intestinal barrier and what cannot. Having a strong intestinal barrier is critical to maintain health as evidenced by a wealth of both animal and human studies.
Most of us also don’t constantly think about our intestinal barrier – but science contends that we should. Because what happens there impacts our entire body and all systems – including our nervous system. A recent study even describes a “Gut Spinal Cord Immune Axis” wherein the health of our spinal cord itself is dependent on immune factors regulated by the gut microbiota. (3) That’s how far your gut health influence goes.
So, let’s talk about one way our gut, a.k.a. microbiome, keeps us healthy. The microbes in our large intestine should be numerous and diverse. These microbes thrive in the presence of prebiotic fiber components (sources of prebiotic fiber are diverse, from the plant world and include things like Jerusalem artichoke, bananas, onions, berries, garlic, and other herbs and spices) which arrive in the colon because they are consumed by the host – us. When your microbes feast on the prebiotic fibers, they produce a by-product, and this byproduct is SCFA’s or short-chain fatty acids. It is well established that these SCFAs play a powerful immunomodulatory role both locally (in the intestine) and distantly (e.g. at the blood-brain barrier). This is the best way to create healthy short-chain fatty acids so they can do what they do best in our system – modulate inflammation.
But what happens if we don’t have richness (as in ample number) or diversity (as in different health-promoting species) of microbes in our large intestine? We can’t produce as many SCFAs.
What happens if we don’t consume the food (eg. prebiotic fiber) our microbes like to eat? Or if we aren’t eating foods that contain microbes (eg. cultured foods)? We can’t produce as many SCFAs.
What happens if we are deficient in healthy SCFAs? We may end up with undesirable physiological sequelae such as systemic inflammation. Which can include blood-brain barrier inflammation. (2)
Remember that we have nerves everywhere in our body – centrally and peripherally. If any of the nerves in our body (peripheral nerves), brain (CNS), or gut (ENS) are inflamed, this can be termed neuroinflammation. Neuroinflammation in the CNS leads to blood-brain barrier inflammation resulting in increased permeability – this ultimately allows substances to reach the brain that shouldn’t.
Neuroinflammation is at the root of many of the health sequelae we currently see in non-communicable conditions. (5) Maybe in your patient it manifests as chronic pain. Maybe in your friend, it’s anxiety and depression. Maybe in your aunt it’s MS, your uncle it’s Alzheimer’s. Maybe in your neighbor it’s fibromyalgia. Neuroinflammation has many faces.
When we look at factors that contribute to blood-brain barrier dysfunction, many can be traced to the cumulative effects of a standard American diet and lack of nutrient density. Further, and more ubiquitous – is our unseen exposure to toxicants such as herbicides and pesticides as well as a multitude of other potential cell health disruptors. (1, 4)
Because of the massive implications of human disease states, we need to pay attention to what the literature is telling us about the interconnected nature of health and lifestyle. We must stop polluting our human physiology and we must start feeding ourselves food that isn’t paradoxically decimating our microbiome. It’s that simple. And complicated. At the same time.
Taking a deep breath is the first step. A crucial second step is staring down the truth of our country’s health care and agricultural realities. The third is gaining perspective on what actions each of us can take today – wherever we live, whatever our socioeconomic status, and whatever our current health status. There is much work to do.
I invite you to an opportunity to learn about many actions we can take today and examine nutritional concerns in depth that have implications not only for the population you treat as a pelvic rehab therapist but for yourself, your friends, and your extended human family.
We must prioritize protective health choices. We must care for our gut, propagate healthy short-chain fatty acids, and therefore care for our blood-brain barrier. And subsequently, protect our brain - like we mean it. Because our modern culture will not do that for us. Solving our nation’s health crises will take each of us collectively to make a difference. The health status of our nation can improve – one protected brain at a time.
Join us for our next offering of Nutrition Perspectives for the Pelvic Rehab Therapist scheduled for June 10-11, 2023.
References:
- Abou Diwan M, Lahimer M, Bach V, Gosselet F, Khorsi-Cauet H, Candela P. Impact of Pesticide Residues on the Gut-Microbiota-Blood-Brain Barrier Axis: A Narrative Review. Int J Mol Sci. 2023 Mar 24;24(7):6147. doi: 10.3390/ijms24076147. PMID: 37047120; PMCID: PMC10094680.
- Fock E, Parnova R. Mechanisms of Blood-Brain Barrier Protection by Microbiota-Derived Short-Chain Fatty Acids. Cells. 2023 Feb 18;12(4):657. doi: 10.3390/cells12040657. PMID: 36831324; PMCID: PMC9954192.
- Raue KD, David BT, Fessler RG. Spinal Cord-Gut-Immune Axis and its Implications Regarding Therapeutic Development for Spinal Cord Injury. J Neurotrauma. 2023 Mar 10. doi: 10.1089/neu.2022.0264. Epub ahead of print. PMID: 36509451.
- Sharma T, Sirpu Natesh N, Pothuraju R, Batra SK, Rachagani S. Gut microbiota: a non-target victim of pesticide-induced toxicity. Gut Microbes. 2023 Jan-Dec;15(1):2187578. doi: 10.1080/19490976.2023.2187578. PMID: 36919486; PMCID: PMC10026936.
- Takata F, Nakagawa S, Matsumoto J, Dohgu S. Blood-Brain Barrier Dysfunction Amplifies the Development of Neuroinflammation: Understanding of Cellular Events in Brain Microvascular Endothelial Cells for Prevention and Treatment of BBB Dysfunction. Front Cell Neurosci. 2021 Sep 13;15:661838. doi: 10.3389/fncel.2021.661838. PMID: 34588955; PMCID: PMC8475767.
Nutrition Perspectives for the Pelvic Rehab Therapist

Price: $525.00 Experience Level: Beginner Contact Hours: 17.5 hours
Course Dates: June 10-11, September 16-17, and December 2-3
Description: Participants will be introduced to the latest research in nutrition through immersive lectures and hands-on labs. The course will cover essential digestion concepts, nourishment strategies, and the interconnected nature of physical and emotional health across the lifespan. Further, clinicians will delve into nutritional relevancies in bowel and bladder dysfunction, pelvic health, pain, and healing. Labs throughout include insightful demonstrations and breakout sessions. The course participant will acquire new, readily applicable tools for patient empowerment, engagement, and self-management utilizing presented principles.

Aparna Rajagopal, PT, MHS, WCS, PRPC, Capp-OB Certified is the lead therapist at Henry Ford Macomb Hospital's pelvic dysfunction program, where she treats pelvic rehab patients and consults with the sports therapy team. Her interest in treating peripartum patients and athletes allowed her to recognize the role that breathing plays in pelvic dysfunction.
Leeann Taptich DPT, SCS, MTC, CSCS leads the Sports Physical Therapy team at Henry Ford Macomb Hospital where she mentors a team of therapists. She also works very closely with the pelvic team at the hospital which gives her a very unique perspective of the athlete.
Aparna and Leeann co-authored the course, Breathing and the Diaphragm: Pelvic and Orthopedic Therapists, which helps clinicians understand breathing mechanics and their relationship to the pelvic floor.
Abdominal bloating and distension are two very commonly reported GI symptoms in the pelvic practice setting. However, these symptoms are not commonly recognized in other physical therapy settings. While many people experience occasional bloating/discomfort it does not necessitate medical intervention, but repeated and long-standing bloating/distention can impact the quality of life.
One diagnosis which is associated with these symptoms is Abdomino-Phrenic dyssynergia where patients develop a paradoxical abdomino-phrenic response. Normally, as a response to an increase in intraluminal gas, the diaphragm relaxes, and the abdominal musculature contracts. When dyssynergia is present, the opposite happens and the diaphragm contracts, and the abdominals relax. Abnormal pelvic floor function is also associated with this diagnosis. Treatments typically used are biofeedback therapy and breathing techniques.
Where Leeann and I work, we are seeing patients increasingly referred with this diagnosis. Recently we treated a 72-year-old female patient with a long-standing history of troublesome bloating and distention, with the diagnosis of Abdomino phrenic dyssynergia.
- The patient had complaints of bloating and abdominal distension all day long, worsening toward evening
- She reported limiting her food intake in the evenings on account of the discomfort and "tightness" in the abdomen
- She rated the discomfort as 3-5/10 in the morning time with an increase to 8/10 by late evening
- She also reported poor sleep because of how "hard and tight" the abdomen felt by bedtime
Upon examination, amongst other findings, the patient demonstrated:
- Significant tightness in her posterior chain and her erector spinae in both thoracic and lumbar regions
- Decreased thoracic rotation/mobility
- Increased connective tissue restrictions in both upper abdominal quadrants, especially in the epigastric area and inferior to the rib cage
- Decreased lower rib cage mobility
- Poor ability to prolong exhale or to exhale strongly
- Decreased ability to relax the pelvic floor musculature after a contraction
In addition to biofeedback and visceral mobilizations, treatment techniques included joint mobility techniques inclusive of simple rib and thoracic spine mobilizations, soft tissue mobility techniques including gentle diaphragm releases, breath training, and breathing techniques to aid in pelvic floor relaxation.
The patient received 9 treatment sessions and a home maintenance program which she followed with good compliance. She reported a 70% overall improvement and was now able to sleep through the night and eat in the evenings without discomfort.
In our course, Breathing and the Diaphragm: Pelvic and Orthopedic Therapists, you will learn:
- Explain normal diaphragmatic breathing and the role of the internal and external oblique musculature.
- Assess and treat dysfunctional breathing patterns including but not limited to chest, abdominal, and paradoxical breathing patterns.
- Understand the concept of Intra-Abdominal Pressure (IAP) and the control and use of IAP with the diaphragm in a lowered position as a stabilizing mechanism for the spine.
- Understand the concept of regional interdependence and its application in the treatment of back or pelvic pain patients.
- Recognize the effects of postural patterns and the linkage to the diaphragm and pelvic floor.
- Understand the muscles and myofascial components involved in dysfunctional breathing and techniques to effectively treat the same.
- Understand and demonstrate mobilizations of the rib and thoracic spine and develop a comprehensive treatment program.
- Develop an exercise progression for dysfunctional breathing for use in the clinic and in-home programs.
- Integrate diaphragmatic breathing and mobility in the athletic clientele
Course Dates: April 22-23
Price: $450
Experience Level: Beginner
Contact Hours: 14
Description: This remote course is an integrated approach where participants will learn how the diaphragm, breathing, and the abdominals can affect core and postural stability through intra-abdominal pressure changes while looking at structures from the glottis and the cervical region to the pelvic floor.
This course includes assessment and treatment of the barriers by addressing thoracic spine articulation and rib cage abnormalities in the fascial system of muscles related to breathing and the diaphragm. Instructed techniques are applicable to patients who present with Diastasis Rectus Abdominis, pelvic pain, incontinence, and prolapse, as well as cervical, thoracic, scapular, and lumbar pain.

Allison Ariail, PT, DPT, CLT-LAANA, BCB-PMD is one of the creators of the Herman & Wallace Oncology of the Pelvic Floor Course Series. Allison Ariail is a physical therapist who started working in oncology in 2007 when she became certified as a lymphatic therapist. She worked with breast cancer, lymphedema patients, head and neck cancer patients, and the overall oncology team to work with the whole patient to help them get better. When writing these courses, Allison was part of a knowledgeable team that included Amy Sides and Nicole Dugan among others.
March is Colorectal Cancer Awareness Month. Did you know that the incidence rate of colorectal cancers is increasing? According to the International Agency for Research on Cancer, 1.9 million new cases of colorectal cancer were identified worldwide in 2020. This number is expected to grow even more. It is predicted that by 2040 the number of new cases of colorectal cancer will rise to 3.2 million new cases a year, and 1.6 million annual deaths worldwide. Additionally, did you know due to the fact that the incidence rate is increasing and it is being diagnosed in younger individuals, the age for screening for colorectal cancer has lowered to 45? At age 45 individuals should begin regular screening for colorectal cancer either via stool-based testing or visual-based screening via a colonoscopy. If someone has risk factors they may need to begin screening at a younger age.
Colorectal cancer can often be preventable through modifiable risk factors. Changing some of these risk factors, alongside the detection and removal of precancerous lesions can lower someone's risks. However, if a diagnosis is made, treatment can help to prolong the life of the patient. The treatment can include various surgeries, chemotherapy, and radiation. All of these treatments can cause changes to a patient's body. A rehab professional that has knowledge about both the body and how the medical treatment of cancer causes changes, can make all the difference in the world for that patient returning to activities that they enjoy and love after treatment.
There are not many opportunities for rehab professionals to learn about these changes and how we can help these patients. However, Herman & Wallace has a series focused on helping oncology patients. In this series, techniques are learned that can help colorectal cancer patients recover from their diagnosis and the medical treatment they go through. The oncology series is online and offered several times a year. You can attend the upcoming oncology courses on: Oncology of the Pelvic Floor Level 1 scheduled for July 8-9 and December 2-3, Level 2A scheduled for May 20--21, and Level 2B scheduled for December 9-10.
Reference:
Morgan E, Arnold M, Gini A, et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Colon. 2023; 72(2).
*Certified Lymphatic Therapists may skip Oncology of the Pelvic Floor Level 1 and move on to the Level 2A and Level 2B courses.*
Oncology of the Pelvic Floor Level 1 - no partner needed for registration
Price: $550.00 Experience Level: Beginner Contact Hours: 17.5 hours
The course will address issues that are commonly seen in a patient who has been diagnosed with cancer such as cardiotoxicity, peripheral neuropathy, and radiation fibrosis. Some holistic medicine topics, including yoga and mindfulness, will be discussed in order to fully prepare the participant to be able to competently work with cancer survivors.
The basics of the lymphatic system will be covered, as well as when to refer the patient to a lymphatic specialist for further treatment. Red flags and warning symptoms will be discussed so the participant feels comfortable with knowing when to refer the patient back to their medical provider for further assessment.
This introductory course is aimed to get the participant comfortable with working with oncology patients and as part of an interdisciplinary oncology team.
Course Dates: July 8-9 and December 2-3
Oncology of the Pelvic Floor Level 2A - partner needed for registration
Price: $495.00 Experience Level: Intermediate Contact Hours: 17.25 hours
This course was designed to build on the information that was presented in Oncology of the Pelvic Floor Level 1.
Information will be provided focusing on male pelvic cancers, colorectal cancer, and anal cancer including risk factors, diagnosis, and prognosis. The participant will also understand the sequelae of the medical treatment of cancer and how this can impact a patient's body and quality of life. Other topics include rehabilitation and nutritional aspects focusing on these specific cancers, as well as home program options that patients can implement as an adjunct to therapy.
Course Dates: May 20--21
Oncology of the Pelvic Floor Level 2B - partner needed for registration
Price: $600.00 Experience Level: Intermediate Contact Hours: 19.25 hours
This course was designed to build on the information that was presented in Oncology of the Pelvic Floor Level 1.
Information will be provided focusing on gynecological and bladder cancers including risk factors, diagnosis, and prognosis. The participant will also understand the sequelae of the medical treatment of cancer and how this can impact a patient’s body and quality of life. Other topics include rehabilitation and nutritional aspects focusing on these specific cancers, as well as home program options that patients can implement as an adjunct to therapy.
Course Dates: December 9-10
All Upcoming Continuing Education Courses

Pelvic Function Level 2B - Satellite - Seattle WA - April 27 - 28 2024 SOLD OUT
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Cranford NJ - April 27 - 28 2024 - SOLD OUT
Apr 27 2024 - Apr 28 2024

Menopause Transitions and Pelvic Rehab - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024

Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024


Pelvic Function Level 2B - Satellite - Des Plaines IL - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024



Pelvic Function Level 2B - Satellite - Hilton Head SC - April 27 - 28 2024
Apr 27 2024 - Apr 28 2024












Pelvic Function Level 1 - Satellite - Kankakee IL - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 1 - Satellite - Wichita KS - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 1 - Satellite - Ann Arbor MI - May 4 - 5 2024 - SOLD OUT
May 4 2024 - May 5 2024

Pelvic Function Level 2B - Satellite - Fairfax VA - May 11 - 12 2024 SOLD OUT
May 11 2024 - May 12 2024


Trauma Awareness for the Pelvic Therapist - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024

Pelvic Function Level 2B - Satellite - East Greenwich RI - May 11 - 12 2024
May 11 2024 - May 12 2024


Sacral Nerve Manual Assessment and Treatment - Remote Course - May 11 - 12 2024
May 11 2024 - May 12 2024


Mobilization of Gastrointestinal Visceral Fascia Satellite Lab Course - Self-Hosted - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Torrance CA - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointesti System Satellite Lab Course - Bedford NH - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System - Asheville NC - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Lansing MI - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course - Scarborough ME - May 17 - 19 2024
May 17 2024 - May 19 2024

Mobilization of Visceral Fascia: Gastrointestinal Satellite Lab Course - Medford OR - May 17 - 19 2024
May 17 2024 - May 19 2024

Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - May 18 - 19 2024
May 18 2024 - May 19 2024

Pelvic Function Level 1 - Satellite - Phoenix AZ - May 18 - 19 2024 - SOLD OUT
May 18 2024 - May 19 2024