Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
The postpartum woman may be one of the most overlooked clients in health care. Knowing the specific rehabilitation needs to help with common problems and to prevent future problems is the goal of this 2-day beginner level course. For the orthopedic-based practitioner, this course will solidify awareness of common orthopedic needs for the postpartum client. For the non-orthopedic practitioner, this course will provide a foundation for working with the client experiencing common postpartum-related musculoskeletal conditions. The course will open with brief case scenarios that highlight the difference between examination/evaluation in the postpartum vs. non-postpartum population. Labor and birth,birth complication and injuries, postpartum stages and concerns, and Cesarean birth all set the stage for the postpartum client and will be reviewed. Understanding typical hormonal and systemic recovery and return to “normal” during postpartum will be provided, including early postpartum changes in the endocrine, metabolic, cardiovascular, pulmonary, immune, neurologic/sensory, integumentary, gastrointestinal, urinary/renal, reproductive, and musculoskeletal systems.
This course will cover examination considerations and modifications specific to postpartum, as well as specific questions to ask during history taking and methods for identifying red flags in postpartum. More comfortable positions during the examination/treatment and common posture/gait/balance changes during postpartum are covered. The participant at this course will understand necessary biomechanics training for daily activities, child care, and breastfeeding. As an expansion from the pregnancy rehabilitation course, participants will be taken through progression in diastasis rectus abdominis (DRA) assessment and rehabilitation, including DRA exercises in lecture and lab. Additionally, addressing abdominal wall lengthening and Cesarean scars will be discussed and practiced in lab.
Overview of pelvic floor dysfunction in the postpartum after vaginal birth with external examination techniques will be expanded from the techniques taught during the pregnancy course. Basic bladder and bowel instructions/education for the postpartum client will be provided, along with guidance on when to refer to a pelvic physical therapist. As an advancement from the pregnancy rehabilitation course, progression in assessment and cueing of pelvic floor, transverse abdominis, and multifidus (deep core) muscle activity will be covered in lecture and lab. Lecture and lab will also address assessing and treating abdominal wall trigger points. Providing instruction and treatment in functional use of abdominal muscles with motor control and functional activities and progression of DRA/abdominal wall rehabilitation exercises will be incorporated into lecture and lab activities.
Basic orthopedic focus on common thoracic and cervical/head complaints in the postpartum will be explored during lecture and lab. This course will also briefly review breathing techniques covered during the pregnancy course. Additionally, discussion and lab practice of lumbar and pelvic girdle examination and treatment techniques in the postpartum will expand on topics covered during the pregnancy rehabilitation course. Review and lab practice will be provided for basic examination and treatment of lower and upper extremity birth and labor injuries.
Psychosocial considerations during postpartum will be explored: the “typical” postpartum patient; postpartum depression, anxiety, and psychosis; postpartum recovery after bedrest; collision of reality and expectations; and maternity leave and return to work decisions. Postpartum exercise, fitness, and wellness will ponder the topics of body image and return to fitness and starting exercise in the postpartum. The course concludes with discussion of marketing and billing needs for providing care for the postpartum population.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: None
Are you interested in expanding your practice to treat prenatal patients? Herman & Wallace has put together a Pregnancy and Your Pelvic Floor marketing presentation to help you underscore the importance of prenatal physical therapy.
References
Gutke, A., Ostgaard, H. C., & Oberg, B. (2006) Pelvic girdle pain and lumbar pain in pregnancy: a cohort study of the consequences in terms of health and functioning. Spine, 31(5), E149-E155. Ostgaard, H. C., Anderson, G. B. J., & Karlson, K. (1991). Prevalence of back pain in pregnancy: A review. Spine, 16(5), 549-552.
Day One: 7:30 Registration 8:00 Introduction, Goals, and Objectives 8:15 Overview of the Postpartum Client 9:00 Hormonal and System Changes and Recovery During Postpartum 9:45 Break 10:00 Abdominal Wall: Diastasis Rectus Abdominis and Post-Cesarean 11:00 LAB: Abdominal Wall Assessment and Scar Treatment 12:00 Lunch 1:00 General Examination Considerations for the Postpartum Client 1:30 General Treatment Considerations for the Postpartum Client 2:15 Pelvic Floor Postpartum 3:15 Break 3:30 LAB: Deep Core and DRA Rehabilitation Progression 4:45 Upper and Lower Quarter Concerns in the Postpartum 5:30 Day 1 Post Test and Wrap Up 6:00 Adjourn
Day Two: 8:00 Examination and Evaluation of Lumbar Spine and Pelvic Girdle in the Postpartum 9:00 LAB: Lumbar Spine and Review of Pelvic Girdle Testing and Treatment 10:00 Break 10:15 Examination, Evaluation, and Treatment of Cervical and Thoracic Spine in the Postpartum Client 11:00 LAB: Cervical and Thoracic Spine Examination and Treatment in the Postpartum Client 11:45 Lunch 12:30 Psychosocial Considerations During Postpartum 1:30 Postpartum Exercise and Fitness 2.06 2:30 Interactive Case Studies 3:15 Marketing and Billing 3:45 Day 2 Post Test and Wrap Up 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to: 1. Define common terminology of the labor and delivery and the postpartum period. 2. Describe the physiologic changes in the postpartum period that assist a woman's body in returning to pre-pregnancy state. 3. List the endocrine system changes, including the risk for thyroid dysfunction, that influence the female patient during the postpartum period. 4. Define the stages of labor, common complications of labor and delivery, and the postpartum red flags. 5. Describe common clinical presentations for perineal trauma and pelvic floor dysfunction. 6. List indications and potential complications of c-section deliveries, as well as principles of c-section recovery. 7. List 2 common conditions and recommended treatment for the spine and trunk, abdomen, pelvic floor, pelvic girdle, upper and lower extremities during the postpartum period. 8. Instruct the postpartum patient in safe return to fitness activities. 9. Describe the challenges that new mothers face and instruct in practical strategies for body mechanics, sleep hygiene, and time management for postpartum recovery. 10. Complete medical screening for conditions in postpartum that require referral.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Arlington, VA - September 18-20, 2020
{dtregister}844{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
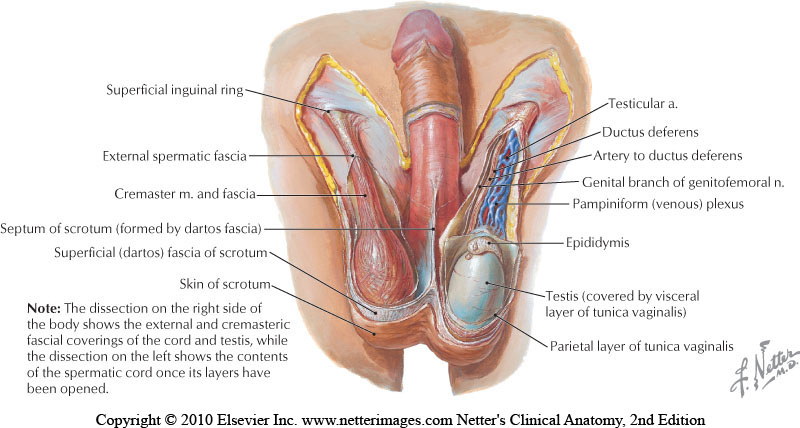
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
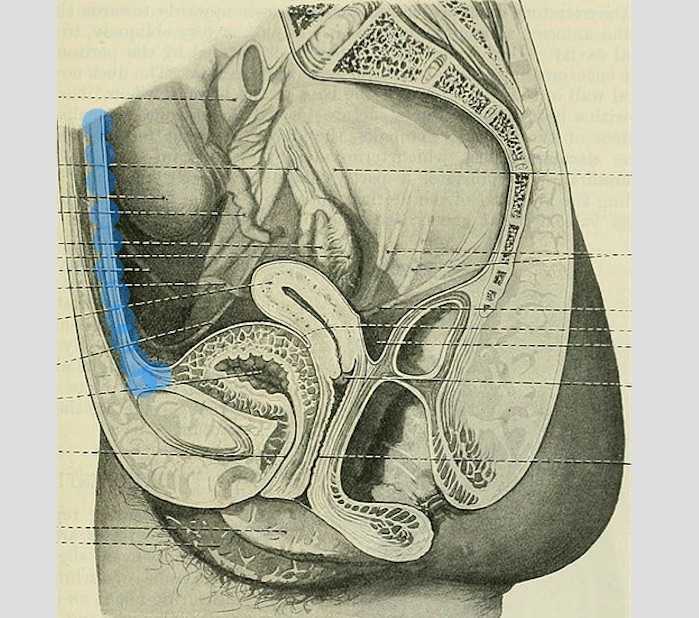
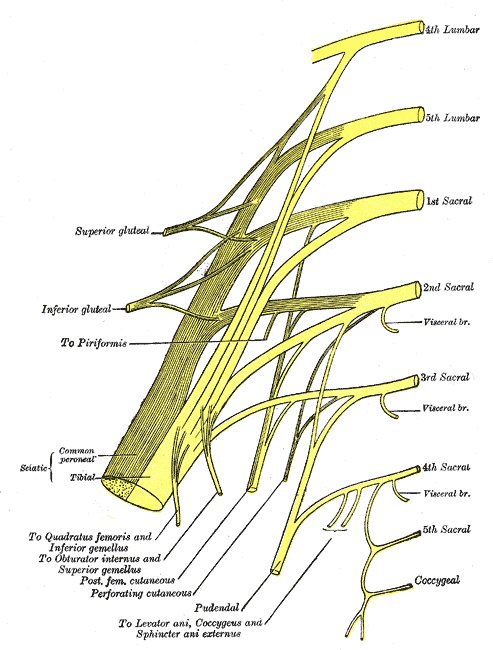
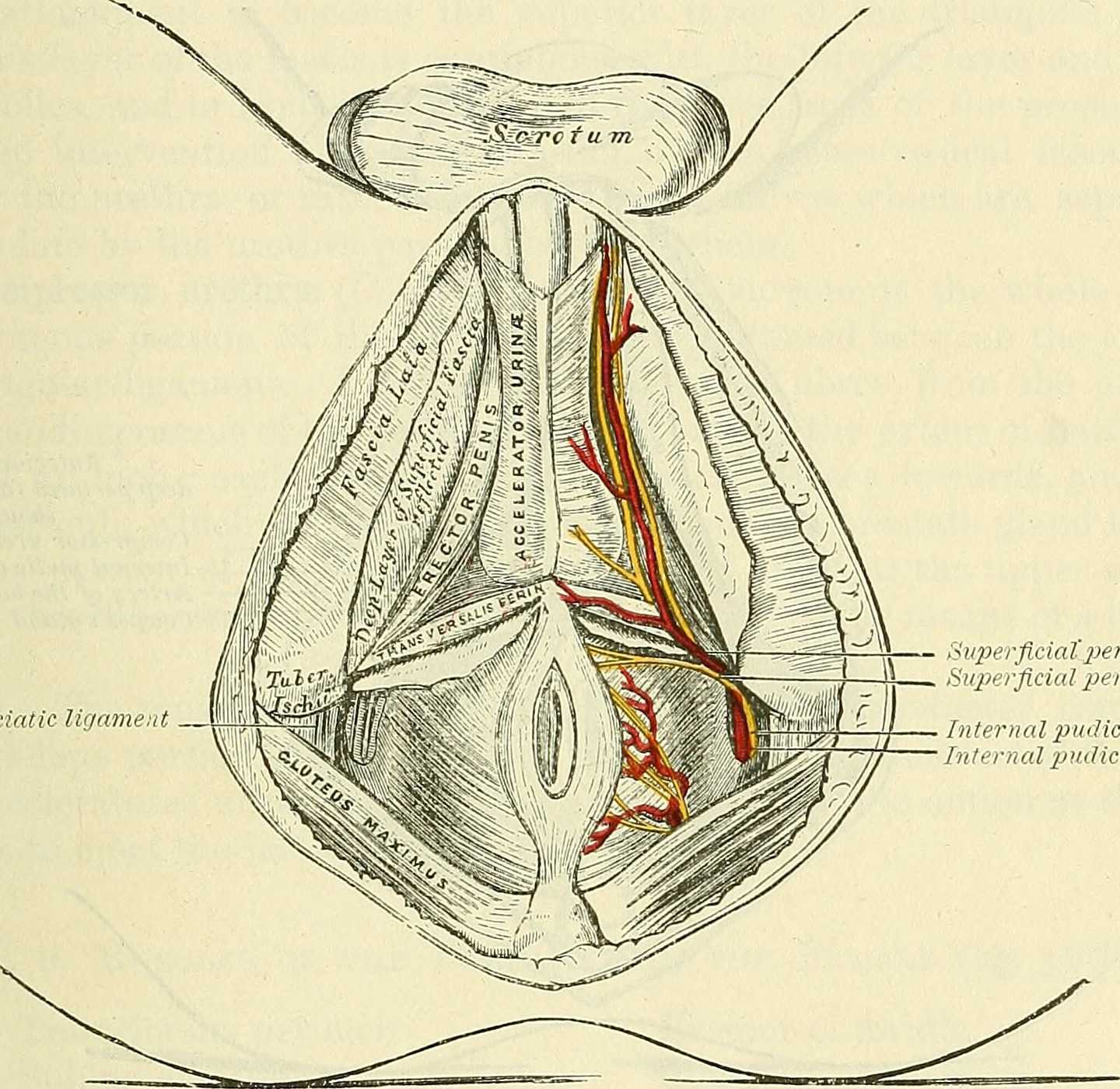
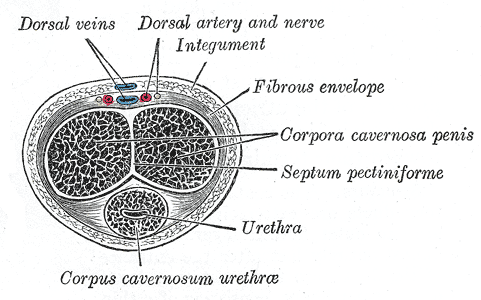
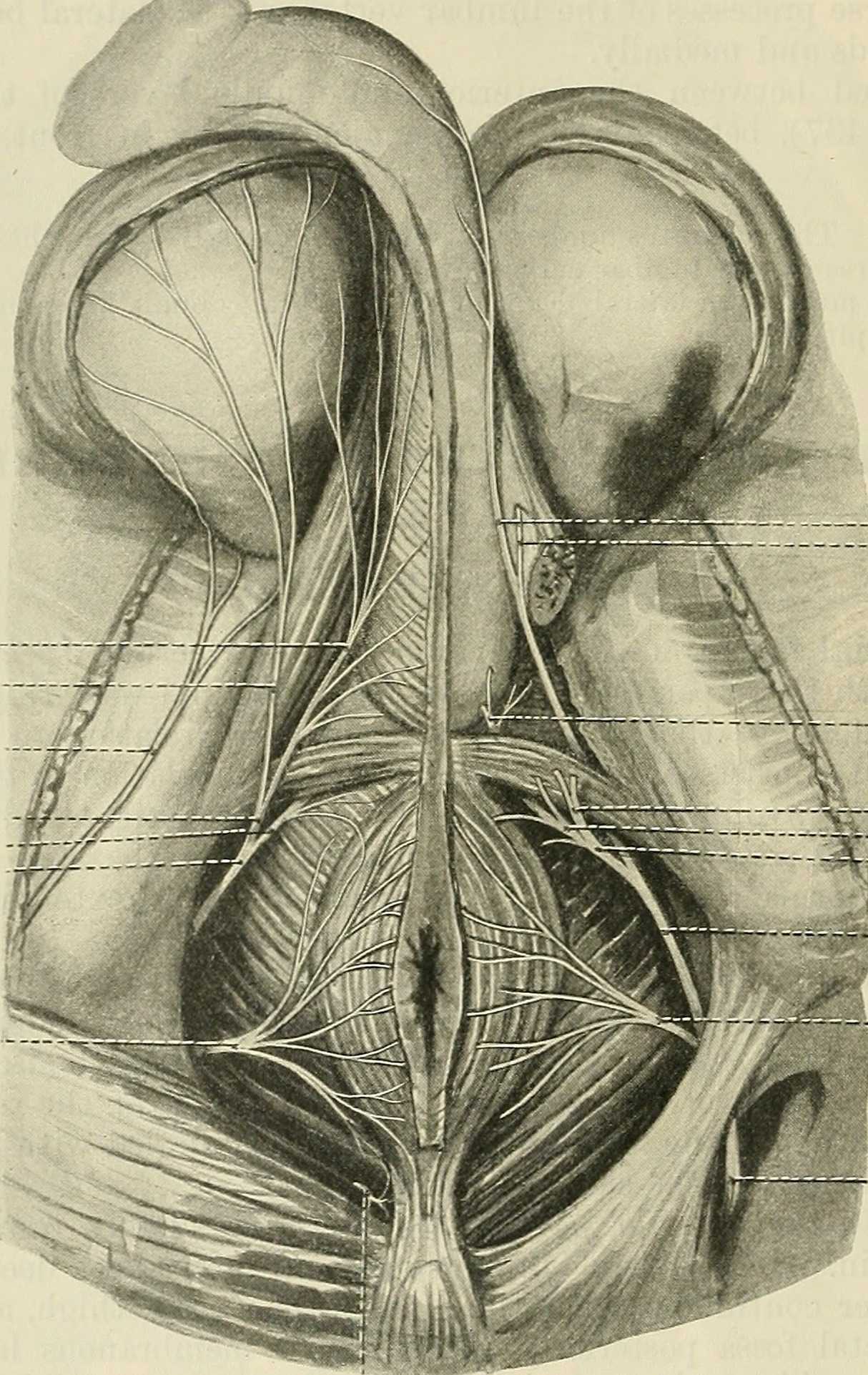
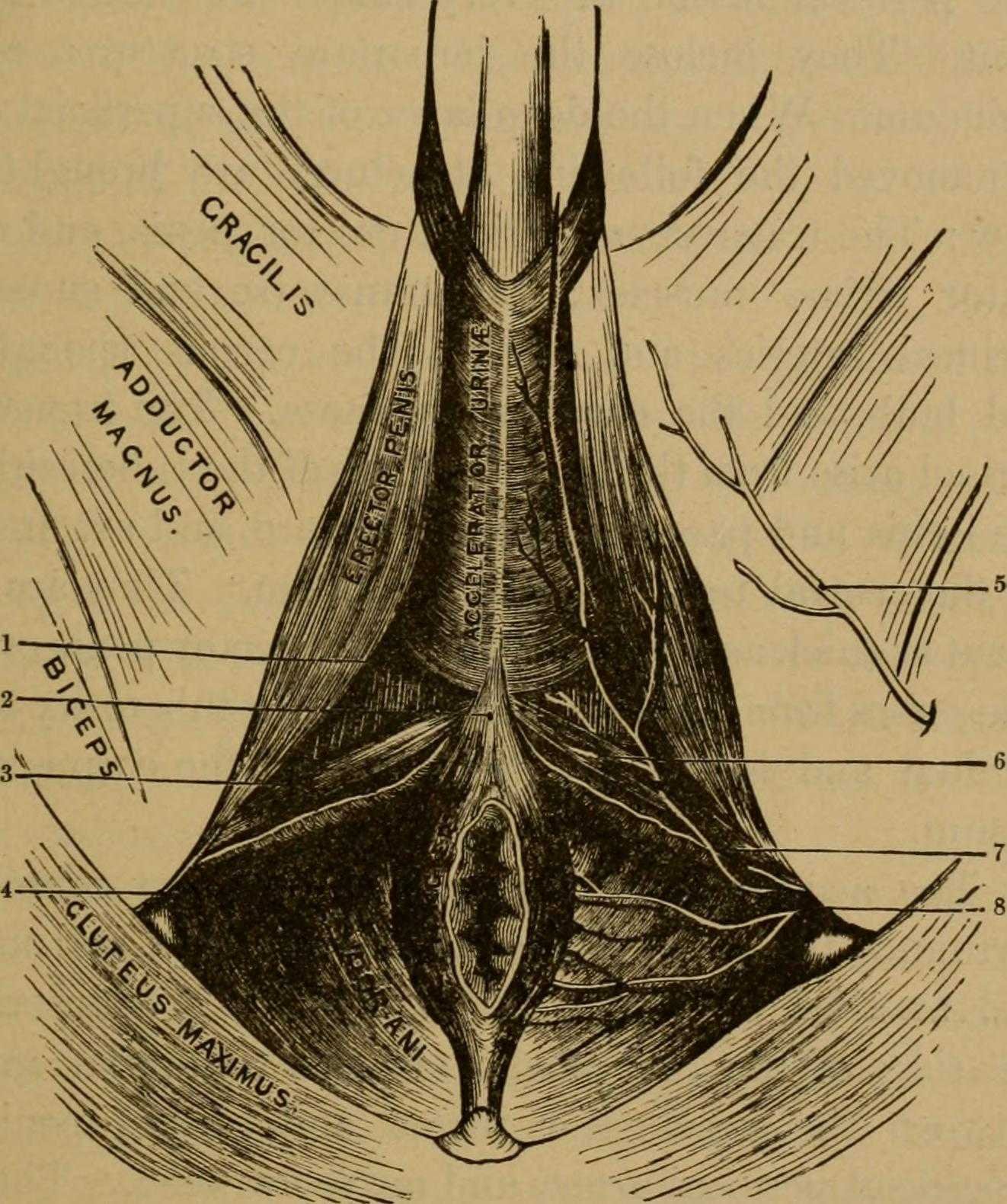
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Colorado Springs, CO - October 3-4, 2020 8AM MDT
{dtregister}908{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructor
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
7:45 Questions from Day 1 8:00 Anatomy of Pelvic Pain 8:45 Pelvic Pain 10:00 Break 10:15 Rehabilitation of Pelvic Pain 11:30 Lunch 12:15 Lab 3: Pelvic Pain Treatment 1:45 Break 2:00 Pathways in Healing 3:00 Question, Wrap-up 3:30 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary rentention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Freehold, NJ - June 15-17, 2018
{dtregister}597{/dtregister}
Description
Schedule
Objectives
Instructor
Location/Lodging
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Grand Rapids, MI - October 27-29, 2017
{dtregister}466{/dtregister}
{gallery width=181}course_images/mpf{/gallery}
Description
Schedule
Objectives
Instructor
Location/Lodging
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Houston, TX - September 14-16, 2018
{dtregister}556{/dtregister}
Description
Schedule
Objectives
Instructor
Location/Lodging
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary rentention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Directions from Recommended Lodging to Course Location:Click here if map is not shown below.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary rentention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Pasadena, CA - September 13-15, 2019
{dtregister}809{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Portland, OR - February 3-5, 2017
{dtregister}475{/dtregister}
{gallery width=181}course_images/mpf{/gallery}
Description
Schedule
Objectives
Instructor
Location/Lodging
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Male Pelvic Floor - Seattle, WA - January 11-13, 2019 (SOLD OUT)
{dtregister}682{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor - Seattle, WA - January 11-13, 2019 (SOLD OUT)
{dtregister}682{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction, & Treatment introduces valuable concepts in male pelvic health including urinary function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Male Course expands on the male pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary rentention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and the recent changes in recommended medical screening and interventions are referenced.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis is a common diagnosis within male chronic pelvic pain. The Male Course explains typical presentations of prostatitis-like pain, evaluation techniques and evidence-informed intervention techniques. Other male pelvic pain diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and male sexual health, including the high-level evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lecture and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introduction, and categories of male pelvic dysfunction 9:00 Male Anatomy Overview, Anatomy, Physiology and Functions of the Male Urinary System 10:00 Break 10:15 Male Urinary Dysfunctions and Medical Examination 11:30 Lecture & Lab Male Pelvic Floor Muscle Strength and Tone Testing, Identification of landmarks 12:30 Lunch 1:30 Physical Therapy Evaluation and Rehabilitation of Male Urinary Dysfunction 2:30 Male Urinary Dysfunction Case Study 3:15 Break 3:30 Anatomy and Physiology of the Male Reproductive System 4:15 Male Sexual/Reproductive Dysfunctions and Medical Examination 5:00 Break 5:15 Rehabilitation for Male Sexual Dysfunction 5:45 Questions/Wrap-Up 6:00 Adjourn
Day Two: 8:00 Review 8:15 Male Pelvic Pain: Musculoskeletal 9:15 Male Pelvic Pain Dysfunctions and Medical Examination 10:30 Break 10:45 Physical Therapy Evaluation and Rehabilitation of Male Pelvic Floor Pain 11:45 Male Pelvic Floor Muscle Mapping 12:45 Lunch 1:15 External Connective Tissue Treatments for Male Pelvic Pain (psoas release, skin rolling, ischiorectalfossa release) 2:15 Pelvic Pain Case Study 2:45 Marketing, Billing, and Questions/Wrap-Up 3:30 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor - St. Paul, MN - April 3-5, 2020 (Rescheduled)
Update 3/19/2020: As a precaution against the spread of COVID-19, this course has been postponed. Once we have a new date confirmed, we will update our website and make the event available for registration. We appreciate your understanding during this difficult time. Please practice good hygiene, and be safe!
{dtregister}867{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course ) Experience Level: Beginner-Intermediate Contact Hours: 22
The Men’s Pelvic Health & Rehabilitation course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in PF2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations:
As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
Day One: 8:00 Introductions, Review of Course Goals/Objectives 8:30 Male Pelvic Health Introduction 9:15 Introduction to Male Anatomy 10:15 Break 10:30 Examination & Evaluation 12:45 Lunch 1:45 Lab 1: Male Pelvic Assessment in Sidelying 2:30 Male Urinary Dysfunction 3:30 Break 3:45 Prostate Conditions 4:45 Questions, wrap-up 5:15 Adjourn
Day Two: 8:00 Questions 8:15 Rehabilitation of Male Urinary Dysfunctions 10:15 Break 10:30 Supine Examination Skills 11:15 Lab 2: Supine Pelvic Floor and Perineal Assessment 12:00 Sexual Function & Dysfunction 12:30 Lunch 1:30 Sexual Function & Dysfunction 3:15 Break 3:30 Rehabilitation of Sexual Dysfunction 5:00 Questions, wrap-up 5:15 Adjourn
Day Three: 7:30 Questions 7:45 Pelvic Pain 9:45 Break 10:00 Pelvic Pain 11:00 Rehabilitation of Pelvic Pain 12:00 Lunch 12:30 Rehabilitation of Pelvic Pain 1:00 Lab 3: Pelvic Pain Treatment Skills 2:00 Break 2:15 Special Topics: Circumcision, Hernias, Testicular Pain 2:45 Pathways in Healing 3:15 Questions, Wrap-up 3:30Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Start Date/Time and Time Zone:
Oct 22, 2022 8:30 AM America/Chicago
Location
Venue: Advocate Good Samaritan Health and Wellness Center
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
All H & W courses have been phenomenal. Good humor, great stories, tons of useful resources, always leave feeling like I have tools to be a more competent PT. - Kristen Parisi, PT, DPT - Bonita Springs, FL
I recently took (*passed) the PRPC exam in May. My preparation for the exam gave me an opportunity to really dive in and understand the content I’ve learned at various H & W courses. The male pelvic course is my first since taking the PRPC, and could really follow along 7 connect the dots more easily. - Kristen Parisi, PT, DPT - Bonita Springs, FL
Great course – instructors and TAs were knowledgeable and willing to help. The course was written in a way to accommodate people already treating this population or people who are looking to add to their patient population. - Karrie Thompson, PT, DPT - Crestview, FL
Holly provided a clinical perspective on the examination of the male pelvic floor. I came into the course without a lot of knowledge on the perineal area of the male and now I feel very comfortable heading back to the clinical and treating this population. - Elizabeth Templeton, PT, DPT - Cape Coal, FL
Thank you, Holly and team, for a meaningful learning experience. Excellent diversity of topics, stimulating conversations and clinically effective manual skills reviewed/progressed. With gratitude! -Allison M Hammond, PT, DPT - Seattle, WA
This was my first pelvic floor course and I never felt lost or that I was falling behind. The course was laid out very smoothly and easy to follow. I learned a lot. -Kaitlin McCaleb, DPT - Houston, TX
I was terrified to make the jump from ortho/sports to the crucial inclusion of pelvic floor in my practice. The lab content has intimidated me since PT school. Thank you for making this accessible and promoting a safe environment. I can’t believe how not scary it was. Amazing content, course and instructors! -Samantha Letizio, PT, DPT, OCS, CSCS - Sneads Ferry, NC
This was a very informative course. I will start utilizing this information as soon as I return to the clinic. Holly was a fantastic instructor. -Maria Drews, PT - Katy, TX
Holly is an excellent teacher – she has a calm and engaging way of presenting the material, answers all questions in a welcoming way and fosters confidence. It is a necessary course to take when treating male patients. It was eye opening and will allow me to advance my skill in the clinic can’t wait to put these strategies to use! -Sarah Snyder, PT, DPT - GREENVILLE, SC
Instructors are always very professional and mature always create an environment that’s extremely comfortable to be in as a learner as a subject during labs. -Aaron Small, PT - Atlanta, GA
I extremely enjoyed this class, it has given me knowledge and confidence need to begin treating men in my clinical practice. I appreciate the emphasis on meeting the patient and their issues uniquely where they are respecting our own bandores. Thank You! -Cora Hargis, DPT - Grand Rapids, MI
Holly is so graceful in her ability to handle difficult, controversial topics + in her language. I am so inspired+excited to treat men begin my journey as a pelvic specialist. -Victoria Snell, DPT - Denver, CO
Holly was absolutely fantastic! This course is fantastic for anyone who treats or wants to treat the male pelvic floor. It is a great resource for both begining and experienced pelvic therapists and provides a remarkably comfortable environment for both men and women. -Jessica Probst, PT,DPT,MTC,SMAC - Washington, DC
Few courses revolutionize my thinking and open endless opportunities to help my patients and this is one of those courses!! This course and Holly challenge your self limits and beliefs in a very open and safe environment with encouragement to think outside the box. -Charles Dudley, MPT - Essex, MD
I feel more confident and knowledgeable to treat the male pelvic pain patient, and also some techniques and info that I can also use on my female patients. I feel that I could take five more courses on this and still learn more! -Audrey Quanrud, PT - Champlin, MN
Such a valuable course for anyone involved in the treatment of male pelvic floor conditions. Very comprehensive and the emphasis on lab and palpitation skills was so helpful. -Kira Boyd, MSPT, ATC- Jacksonville, NC
Even though the focus of my practice is on pelvic health, I learned quite a bit about external palpitation skills. The adaptation of women to men was very helpful. -Lori Buxton, PT, DPT, WCS - Littleton, CO
This has been such an amazing course and I feel I can really treat all male patients. I feel there is so much more to develop in my male pelvic floor treatment program and I can educate my referring providers. -Caitlin Ruggiero DPT - Bishopville, MD
I never thought I'd be excited to provide male pelvic floor rehab, but after this course I realize that like female pelvic floor, male pelvic floor is very under-served. This motivated me to expand my practice. -Cynthia Kakuk Marchi, OTR/L - Alburquerque, NM
Great course! [This is my] second course taken with Holly and Stacey and they are by far my favorite presenters!!! I gained so many tools! Excited to learn more about past vesiculate surgeries, hernia repair, etc. -Natalie Miller, PTA San Diego, CA
Excellent anatomy review and education regarding medical issues, as well as putting together clinical pieces. I really loved the emphasis on clinical reasoning to figure out what each individual needs, no protocols etc. Thank you! - Anonymous This is my very first pelvic floor course and I am very excited about all I learned and am so looking forward to go back to KS and start a program there. -Mario Alarado, MD, PT – Witchita, KS Helped us open up the new horizon. Good course to start a pelvic rehab program. I enjoyed this for the first time it gave me confidence. -Ramesh Malladi, PT, RPT – Livonia, MI Great course with new information and techniques that will help further my “toolbox” and ability to take male patients with pelvic pain. -Amy Walter, DPT – Hamburg, NY I appreciate instructors who are knowledgeable and approachable as well as passionate about their subject matter-Thank You! To Holly and Stacey for a good weekend of learning. Thanks for sharing pt. examples, you are both good speakers! -Kelly Poole, MPT – Bogart, GA This is my second course with Holly and Stacey. They are a great time. Very informative, enthusiastic and passionate. Thank you! -Patti Koehler – Portland, OR Great Course! -Catherine Weibel, DPT, WCS - Winter Park, FL
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course. Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a self-hosted satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. As this course covers the role and function of male anatomical structures, self-hosted registrants would be best served by partnering with someone with male anatomy. This is not a requirement, but please understanding that doing so is advised in order to get the best learning experience. Solo participants may register for this course if they have a lab partner with a scrotum and penis to attend the course with. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hrs, 40 min
1) Pelvic Health Introduction (36 min) 2) Introduction to Anatomy (59 min) 3) Urinary & Prostate (85 min) 4) Sexual Function & Dysfunction (92 min) 5) Pelvic Pain Foundations (72 min) 6) Special Topics (84 min) 7) Starting A Men's Health Program (33 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introductions, Review of Course Goals/Objectives
7:00 - Examination & Evaluation 8:30 - Break 8:45 - Examination & Evaluation 9:15 - Lab 1 Prep: Anorectal Assessment in Side-lying 9:30 - Lab 1: Anorectal Assessment in Side-lying 10:30 - Lunch 11:30 - Rehabilitation of Urinary Dysfunction 1:30 - Break 1:45 - Lab 2 Prep: Supine Pelvic Floor and Perineal Assessment Supine 2:15 - Lab 2: Supine Pelvic Floor and Perineal Assessment Supine 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions 6:45 -Rehabilitation of Sexual Dysfunction 7:45 - Pelvic Pain in Men 8:45 - Break 9:00 - Rehabilitation of Pelvic Pain 11:00 - Lunch 11:45 - Lab 3 Prep: Pelvic Pain Treatment 12:45 - Lab 3: Pelvic Pain Treatment 2:00 - Synthesizing Pain, Continence, Sexual Health 2:30 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
This is a satellite lab course offering of our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Special Considerations: As this continuing education course includes extensive lab work, all attendees should come prepared to participate as both clinician and patient unless medically contraindicated (if unsure please check with your physician prior to attending the course). Internal rectal pelvic floor muscle examinations will be taught in labs. As this is a male course, please be aware that the instructors encourage male attendees. Herman & Wallace seeks to maintain a better than 10:1 student-to-teacher ratio, with in-person lab assistants guiding the hands-on learning.
Audience: This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites: This course is for therapists with experience in treating pelvic floor dysfunction. This course is also appropriate for the practitioner who has not had any training in pelvic floor dysfunction and who is interested in treating male patients. All pre-recorded lectures in Teachable for this course must also be watched before the Live Component of the course. See the Schedule tab for the current list of pre-recorded videos
7:45 Questions from Day 1 8:00 Anatomy of Pelvic Pain 8:45 Pelvic Pain 10:00 Break 10:15 Rehabilitation of Pelvic Pain 11:30 Lunch 12:15 Lab 3: Pelvic Pain Treatment 1:45 Break 2:00 Pathways in Healing 3:00 Question, Wrap-up 3:30 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy and physiology of the urogenital, gastrointestinal, musculoskeletal, fascial and nervous systems with reference to men’s pelvic health and dysfunction. 2. List key medical diagnostic procedures for urologic, sexual and pelvic pain conditions. 3. Perform external and internal (rectal) examinations of the pelvis to identify specific pelvic floor muscles, ligaments, nerves, and key bony landmarks. 4. Perform pelvic floor muscle assessment procedures to identify strength, tone, length and coordination. 5. Demonstrate abdominal wall examination and treatment, and describe abdominal wall as potential role in referral of symptoms to the pelvis. 6. Instruct patients in a home program and behavioral education for urologic, sexual, and pelvic pain conditions. 7. Design treatment plans for chronic pelvic pain syndromes, erectile dysfunction and post-prostatectomy dysfunctions. 8. Perform external and internal pelvic floor myofascial treatment techniques. 9. Identify alternate ways of approaching healing with respect to patient’s experiences and within respective scopes of practice. 10. List resources for patients in regards to appropriate referral to other providers.
Directions from Recommended Lodging to Course Location
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Start Date/Time and Time Zone:
May 20, 2023 9:30 AM America/New_York
Location
Venue: Piedmont Rockdale Rehabilitation and Physical Therapy
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Start Date/Time and Time Zone:
Nov 18, 2023 6:30 AM America/Los_Angeles
Location
Venue: Life in Balance Physical Therapy - Normandy Park Office
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Male Pelvic Floor Function, Dysfunction and Treatment
Course Description
This is a satellite lab course offering our popular Men’s Pelvic Health & Rehabilitation course. The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Level 1 - Detroit, MI - June 7-9, 2019 (SOLD OUT)
{dtregister}761{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner was born and raised in Duluth, Minnesota, and has lived in Washington state for most of her adult life. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and in Pelvic Rehabilitation. She teaches continuing education courses nationally, teaches in the transitional Doctor of Physical Therapy program for the College of St. Scholastics, and serves as a consultant for practice and program development. She is a member of the American Physical Therapy Association and the American Massage Therapy Association.
Kimberly M. Glow, PT, DPT is a Boston-based physical therapist with a focus on both pelvic floor dysfunction and orthopedics. Kim graduated with her doctorate in physcial therapy from MGHIHP after completing her undergraduate work in Classics at UNH. She believes in the healing power of movement, and the power of the biopsychosocial connection. She has a passion for seamlessly treating pelvic floor dysfunction and orthopedic dysfunction as inter-related components. As an auspicious educator, Kim has been involved with many community-based education programs, including lectures and demonstrations to local yoga studios during instructor trainings, postpartum support groups, and support groups for those afflicted with neurological disease. In 2017, Kim was invited to guest lecture on the topic of “Physical Therapy’s Role in Treatment of Vulvovaginal Dermatological Conditions” during the American Urogynecologic Society’s annual conference, and has also lectured to medical residents at Tufts Medical Center.
Kimberly has a special passion for treating athletes with pelvic floor dysfunction, and returning them to the sport or movement style they most love. Her practice includes treatment of bowel, bladder, sexual, breast, and abdominal dysfunction for both men and women, as well as all breadths of orthopedic dysfunction. She has a passion for lifelong learning, and education. Currently, Kimberly practices out of Massachusetts General Hospital.
Kim enjoys her spare time with her husband and puppy, camping, and reading. Kim currently practices out of Rhode Island.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Jessica Reale, PT, DPT, WCS
Jessica is a board-certified specialist in Women’s Health (WCS) and is passionate about working with all people with pelvic floor disorders, especially those with chronic pelvic pain, urinary dysfunction and bowel dysfunction. She is a graduate of Gordon College with a B.S. in Kinesiology and of Duke University where she received her Doctor of Physical Therapy degree. Jessica owns and treats patients at Southern Pelvic Health in Atlanta, GA, a specialty pelvic rehabilitation practice.
Jessica is passionate about pelvic health education, and works closely with Holly Tanner in writing and updating Pelvic Floor Level 1, 2A and 2B coursework. She also regularly guest lectures at local university DPT programs, and has presented at conferences, seminars, community groups, and various medical and physical therapy residency programs.
Jessica loves supporting other pelvic rehabilitation providers, and founded the Facebook group, Pelvic PT Newbies, as a place for safe questioning, learning and growth. She also established and runs a professional small group mentoring program several times each year. She also runs an educational blog on pelvic health topics through her website, and is active on social media @southernpelvichealth, spreading awareness of pelvic floor dysfunction and pelvic rehabilitation. Outside of work, Jessica enjoys spending time with her husband and 2 daughters, staying active, and traveling. .
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Price: $725 (Early Registrant Price of $695 ends one month before the first day of the course). Experience Level: Beginner Contact Hours: 22.5
This continuing education course is a three-day seminar designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Pregnant women course attendees may participate fully in the entire course if they bring their own lab model for examination, or if the attendee insists on lab participation then a clearance letter from their physician allowing them to participate in the labs is required. We strongly recommend that pregnant attendees bring a model as vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. If pregnant participants cannot bring a model, they have the option of working in a group of three during lab times.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Directions from Recommended Lodging to Course Location
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Level 1 - Los Angeles, CA - March 22-24, 2019 (SOLD OUT)
{dtregister}733{/dtregister}
Description
Schedule
Objectives
Location/Lodging
Instructors
Discounts
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Jenni Gabelsberg, DPT, WCS, MSc, MTC, PRPC
Dr. Jenni Gabelsberg, DPT, MSc, MTC is a women's health physical therapist specializing in urinary incontinence and pelvic pain since 1994. She strives to empower patients through education and self-awareness to encourage them to take responsibility for their own health. She believes that a physical therapist's education forms the cornerstone of her care. She attended the University of Vermont and earned a Bachelor of Science, Physical Therapy, in 1994. She went on to earn a Manual Therapy Certification (MTC) awarded by the Institute of Physical Therapy in 1995. Dr. Gabelsberg next earned an Advanced Masters in Orthopedic Physical Therapy from the University of Saint Augustine for Health Sciences in 1999, and a Doctorate in Physical Therapy in 2003.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Level 1 - Medford, OR - June 22-24, 2018
{dtregister}630{/dtregister}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location:
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Start Date/Time and Time Zone:
Apr 29, 2023 6:30 AM America/Los_Angeles
Location
Venue: Life in Balance Physical Therapy - Normandy Park Office
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Level 1 - Richland, WA - August 19-21, 2016
{dtregister}383{/dtregister}
{gallery width=181}course_images/pf1{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price: $725 (Early Registrant Price of $695 ends one month before the first day of the course). Experience Level: Beginner Contact Hours: 22.5
This continuing education course is a three-day seminar designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Pregnant women course attendees may participate fully in the entire course if they bring their own lab model for examination, or if the attendee insists on lab participation then a clearance letter from their physician allowing them to participate in the labs is required. We strongly recommend that pregnant attendees bring a model as vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. If pregnant participants cannot bring a model, they have the option of working in a group of three during lab times.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Level 1 - Seattle, WA - March 17-19, 2017 (SOLD OUT!)
{dtregister}427{/dtregister}
{gallery width=181}course_images/pf1{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
<
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Level 1 - Stockton, CA - January 27-29, 2017
{dtregister}418{/dtregister}
{gallery width=181}course_images/pf1{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Jenni Gabelsberg, DPT, WCS, MSc, MTC, PRPC
Dr. Jenni Gabelsberg, DPT, MSc, MTC is a women's health physical therapist specializing in urinary incontinence and pelvic pain since 1994. She strives to empower patients through education and self-awareness to encourage them to take responsibility for their own health. She believes that a physical therapist's education forms the cornerstone of her care. She attended the University of Vermont and earned a Bachelor of Science, Physical Therapy, in 1994. She went on to earn a Manual Therapy Certification (MTC) awarded by the Institute of Physical Therapy in 1995. Dr. Gabelsberg next earned an Advanced Masters in Orthopedic Physical Therapy from the University of Saint Augustine for Health Sciences in 1999, and a Doctorate in Physical Therapy in 2003.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Price:$695 ($725 within one month of the course) Experience Level: Beginner
This continuing education course is comprised of 9 hours of prerecorded lectures followed by two-days of in-person learning, and was designed to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. It is geared to the physical therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination and SEMG biofeedback assessment. The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, SEMG biofeedback, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. Participants who are pregnant who wish to participate fully in the entire course including in lab must bring a clearance letter from their physician allowing them to participate in the labs is required. Participants who are pregnant also have the option of bringing their own lab model for examination, or they have the option of working in a group of three during lab times.
This course instructs in the use of biofeedback equipment. Equipment at the course will be supplied by our biofeedback vendor, Current Medical Technologies. If you would like to contact them prior to the course to inquire about equipment purchases, you can do so using this link. A representative will be able to assist you if you tell them which Herman & Wallace course you will be taking.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar. We ask that participants keep a personal bladder diary measuring and recording fluid intake and urine output for two days - one work day and one non-work day. Specific measurements (use a large measuring cup or urine collection “hat”) of urine output are needed for at least one day, and on the following day one can estimate by counting seconds while voiding.
7:30 Questions, Post-test Day 2 7:45 Pelvic Organ Prolapse 8:45 Lab 6: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:45 Break 10:00 Specific Diagnoses in Female Pelvic Pain 11:15 Managing Movement Part II: Pressures & Load Transfer 12:00 Lunch 1:00 Managing Movement Part II: Pressures & Load Transfer 1:45 Final Lab Preparation 2:00 Lab 7: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:15 Break 3:30 Case Studies 4:00 Questions (Resources, Billing, Marketing, Etc.), Wrap-up 4:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Teri Elliott-Burke, PT, MHS, BCB-PMD
Teri Elliott-Burke, PT, MHS has been practicing physical therapy since 1978. She received a Masters in Health Science from the University of Indianapolis, a certificate in physical therapy from Northwestern University Medical School and a BA in biology and psychology from North Central College. She is the co-owner of Women’s Physical Therapy Institute, in Lake Zurich, IL specializing in orthopedics and pelvic dysfunction for men, women, and children. She is an adjunct faculty member of Midwestern University in Downers Grove, IL where she co-teaches Management in Physical Therapy Systems, Applied Management Skills in Physical Therapy Systems, and lectures on women’s health and pelvic dysfunction. She is a member of the APTA Section on Women’s Health, the Private Practice Section, the International Pelvic Pain Society, American Urogynecologic Society, and the Chicagoland Pelvic Floor Research Consortium. Teri also speaks frequently to community and professional groups on topics related to pelvic dysfunction for men and women. She strives to maintain a balance between work, her family (1 husband, 2 sons), her church and community.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
This remote continuing education course provides live instruction in foundational content in pelvic floor rehabilitation physical therapy. This course consists of the same content contained in the pre-recorded lectures of Pelvic Floor Level 1. Participants who join us for this remote course will have a chance to experience these lectures live with an HW faculty member, who will answer questions in real time.
Participants may choose to take this course and then sign up for the full-length Pelvic Floor Level 1 course, which includes labs, and is offered in both In-Person and Satellite formats. Participants who sign up for the full Pelvic Floor Level 1 course will receive the pre-recorded lectures of the content contained in this course, which they may use to review. It is therefore NOT required that one take Pelvic Floor Level 1 Part 1 prior to taking the full-length Pelvic Floor Level 1 course. However, this is the perfect option for a therapist who has yet to find a Pelvic Floor Level 1 in their region, and who wants to begin their pelvic rehab training while practicing strict social distancing, or the therapist who is curious to learn more about pelvic rehab but is not yet ready to attend a course inclusive of labs.
Included in the remote course is a thorough overview of pelvic anatomy, concepts and techniques in trunk and pelvic evaluation and examination including the observation and retraining of movement patterns. Lectures will cover specific conditions including urinary incontinence and pelvic pain. Concepts related to trauma-informed care will also be included in this comprehensive introduction. Participants are encouraged to come with questions about starting their journey becoming pelvic rehab practitioners for the instructor.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Please Note: Those who were registered for a Pelvic Floor 1 course which was postponed due to Covid-19, and whose course has not been rescheduled yet, are invited to attend this remote Pelvic Floor 1 Part 1 course at no additional fee. Please contact us to verify eligibility and register if you would like to take advantage of this offer.
Please Contact Us with any questions about the use of this text as a required reading in this course.
Special Considerations: This course will be offered as a live, interactive remote course on Zoom, taught by an instructor who will teach introductory didactic lectures and answer questions.
The times listed are for the afternoon offerings of PF1.1 All times are Pacific Time.
Day One:
12:00 Log on, Zoom basics, introductions, goals, objectives 12:30 Pelvic Floor Anatomy & Function 01:15 Pelvic Floor Evaluation and Examination 02:45 Break 03:00 Managing Movement 04:00 Awareness of Trauma in Pelvic Rehab 05:00 Adjourn
Day Two:
12:00 Questions from Day 1 12:15 Urinary Incontinence 1:45 Break 02:00 Introduction to Pelvic Pain 03:00 General Treatment of Pelvic Pain 04:00 Questionns 04:15 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 5. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 6. Begin to develop evidence-based treatment plans and progressive clinical goals for pelvic floor dysfunctions 7. Recognize key components of trauma-based care
Attending a remote course is easy and safe, and you can do it entirely from the security and comfort of your own home or clinic without having to find a lab partner.
Important thing to note:
- Our policy for applying for continuing education credit for remote courses differs from that of our in-person and satellite lab courses. Read the specific language of the policy here. Depending on the state in which you practice, you may need to submit your own application to your state board or approving body should you wish that it be approved for continuing education credit in your state.
- To attend a remote Herman & Wallace course, registrants will need Zoom video conferencing software. This is a requirement. One can create an account and download the software to their computer at https://zoom.us/
- We use the Pacific Time Zone for all of our remote course start and end times (this is not the case for in-person and satellite lab locations). Please make a note of this and set your calendar accordingly.
- A Zoom account is free to create. Before the meeting, we recommend having a practice Zoom session with a friend or colleague so you can test your microphone, video, and internet connection. You can participate in any remote course from the comfort of your home, but will need a stable internet connection in order to participate. We recommend downloading the software and practicing a call with a friend or colleague prior to your course with us. Zoom also offers video tutorials on their website at https://support.zoom.us/hc/en-us/articles/206618765-Zoom-Video-Tutorials.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
PLEASE NOTE: This location requires that participants bring their own laptop and headphones to each course hosted here. Attendees will participate from treatment rooms in the facility, and will be joining the course Zoom from their personal laptops.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Start Date/Time and Time Zone:
Jul 9, 2022 9:30 AM America/New_York
Location
Venue: Orthopaedics Plus Physical Therapy - Bedford
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
This continuing education course consists of pre-recorded lectures followed by live, interactive remote learning that will be completed by groups meeting at a specific satellite location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location. During labs, participants will pair up and be guided by the on-site lab assistants.
This course was designed to provide a thorough introduction to pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Presentation of evidence-based evaluation and treatment techniques will be emphasized. Outcome measures and quality of life questionnaires will be presented for both urinary incontinence and pain syndromes. Daily lab time allows for supervised instruction of pelvic floor muscle evaluation with external palpation and internal vaginal examination of pelvic floor musculature. For each condition the therapist will learn to: recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities; use an evaluation/outcome tool; and perform a suggested protocol of treatment interventions. Clinical treatment interventions will include therapeutic exercise, external manual therapy, patient related education/behavioral instructions and electrotherapeutic modalities.
Prerequisites
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom All pre-recorded lectures must be completed before attending the first day of class.
Audience
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 10 hours
1) Pelvic Floor Anatomy & Function (51 minutes) 2) Pelvic Floor Evaluation and Examination (1 hour 30 min) 3) Managing Movement (1 hour) 4) Urinary Incontinence (1 hour 30 min) 5) Introduction to Pelvic Pain (1 hour 10 min) 6) General Treatment of Pelvic Pain (1 hour) 7) Awareness of Trauma (1 hour) 8) Pelvic Organ Prolapse (1 hour 10 min) 9) Introduction to Biofeedback and Electrical Stimulation (46 min) 10) Additional Resources on Biofeedback and E-Stim from our Partners at CMT (Optional)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, goals, objectives, questions
6:45 - Pelvic Floor (PF) Anatomy and Evaluation 7:30 - Lab 1: PF Exam Techniques Part 1: Observation, Identification, Muscle layers, ICS Scoring 8:45 - Break 9:00 - Pelvic Floor Evaluation (Continued) 9:30 - Lab 2: PF Exam Techniques Part 2: PF MMT, Laycock Exam, Pelvic Clock, Obturator Internus 10:30 - Lunch 11:30 - Urinary Incontinence Examination & Interventions Part II 1:00 - Break 1:15 - Lab 3: Bladder Diary Activity 2:00 - Questions 2:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 4 Prep, Lab 4: Screening of Breathing & Load Transfer Strategies, Abdominal Wall Dysfunction 7:30 - Break 7:45 - Lab 5: Pelvic Floor Examination and Prolapse Exam, External Palpation 9:00 - Specific Diagnoses in Female Pelvic Pain 10:30 - Lunch 11:00 - Managing Movement Part II: Pressures & Load Transfer 12:45 - Final Lab Preparation Presentation 1:00 - Lab 6: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 2:00 - Break 2:15 - Case Studies 2:45 - Questions (Resources, Billing, Marketing, Etc.), Wrap-up 3:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of recorded lecture videos followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely. We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 1)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 1. This continuing education course consists of 10 hours of recorded lecture videos followed by 14 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. Participants in this event will meet in person to watch the Zoom presentation in the same location and participate in labs together, with the instructor guiding remotely.
We designed this course to provide a thorough introduction to female pelvic floor function, dysfunction and treatment interventions. This course is geared to the therapist who wants to synthesize the information and apply it to individual treatment programs for urinary incontinence or the musculoskeletal components of urogynecologic pain syndromes such as chronic pelvic pain (CPP), vulvar pain, and interstitial cystitis/painful bladder syndrome (IC/PBS). This continuing education seminar teaches evaluation and treatment interventions by instructional assessment of the pelvic floor muscles with internal vaginal examination, and SEMG biofeedback assessment (please note that, for the time being, SEMG is being demonstrated in video lectures; for hands-on learning, consider attending Biofeedback for Pelvic Muscle Dysfunction). The information is immediately applicable to clinical practice.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Level 2A - Bayshore, NY - July 16-18, 2017 (Sold Out)
{dtregister}423{/dtregister}
{gallery width=181}course_images/pf2a{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day (8 hours of online content, followed by a 2-day in-person course) intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Lila Abbate, PT, DPT, MS, OCS, WCS, PRPC
Lila Abbate, PT, DPT, MS, OCS, WCS, PRPC is the Director/Owner of New Dimensions Physical Therapy with locations Roslyn, Long Island, and the Noho Section of New York City. Dr. Abbate graduated from Touro College in Dix Hills, NY with a Bachelors of Science (BS) in Health Sciences and a Masters of Arts (MA) in Physical Therapy in 1997. She completed her Advanced Masters in Manual Orthopedic Physical Therapy (MS) at Touro College, Bayshore, NY in 2003 and continued to pursue her Doctor of Physical Therapy (DPT) at Touro in 2005. Dr. Abbate is a Board-Certified Specialist by the American Physical Therapy Association in Orthopedics (OCS) 2004 and Women’s Health (WCS) 2011. She has obtained the Certified Pelvic Rehabilitation Practitioner (PRPC) by Herman & Wallace Institute, 2014. She is a Diane Lee/LJ Lee, Integrated Systems Model (ISM) graduate and completed the New York series in 2012.
Dr. Abbate has been an educator for most of her physical therapy career. She has experience as full-time faculty at Touro College, Manhattan Campus from 2002 to 2006 teaching the biomechanical approach to orthopedic dysfunction and therapeutic exercise as well as massage/soft tissue work that highlighted trigger point work, scar management, and myofascial release.
She is currently on faculty as a Lecturer at Columbia University teaching the private practice section Business & Management course (since 2016) along with the Pelvic Health elective (since 2012). She teaches nationally and internationally with the Herman & Wallace Pelvic Rehabilitation Institute teaching advanced courses of her own intellectual property: Orthopedic Assessment for the Pelvic Health Therapist, Bowel Pathology Function, Dysfunction and the Pelvic Floor, Coccydynia & Painful Sitting: Orthopedic Implications. She was a co-writer for the Pudendal Neuralgia course and teaches the Pelvic Floor Series of Pelvic Floor 1, 2A and 2B and Pregnancy, Postpartum. She has written two book chapters in 2016: Pelvic Pain Management by Valvoska and Healing in Urology: Clinical Guidebook to Herbal and Alternative Therapies by Chughtai.
She is a member of the American Physical Therapy Association, the National Vulvodynia Association, the American Urogynecology Association, and the International Pelvic Pain Society. Dr. Abbate is also a Senior Physical Therapy consultant for SI Bone, a sacroiliac joint instrumentation company.
Stacey Futterman Tauriello, PT, MPT, WCS, BCB-PMD, PPRC, received her Master’s Degree in Physical Therapy from Nova Southeastern University in South Florida in 1996. After graduation she relocated to Chicago where she began specializing in women’s health issues including the treatment of incontinence, pelvic pain and prenatal/postpartum musculoskeletal issues. She returned to the east coast in 2003 and is now the owner of 5 Point Physical Therapy, a specialty physical therapy clinic for male and female pelvic dysfunction in New York City. Stacey, along side Dr. Deborah Coady, recently presented for International Pelvic Pain Society’s annual meeting in Chicago on their research of hip pathology and its relationship to pelvic pain. She has been featured on CBS New York and has presented for the APTA National Conference 2007 for the treatment of male pelvic pain.
Directions from Recommended Lodging to Course Location:Click here if map is not shown below.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Start Date/Time and Time Zone:
Feb 11, 2023 9:30 AM America/New_York
Location
Venue: Piedmont Rockdale Rehabilitation and Physical Therapy
This is a self-hosted satellite offering of our PF2A course. A satellite course means that the instructor is presently live on Zoom and that participants are gathering in various locations in order to participate and practice labs with one another. Self-hosted means that participants must register in pairs or small groups and practice on each other during lab time.
This continuing education course is comprised of 7 hours and 45 minutes of prerecorded lectures followed by 14 hours of live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
Please note, this is a full lab course that is done remotely. These guidelines represent how we feel you can best experience a remote course. If you feel you are unable to fulfill them then it is recommended that you not participate as a remote learner at this time.
You will need to register with a PT partner. The feedback of your lab partner is highly valuable, therefore you will need to collaborate with another clinician, preferably someone in your clinic or health system that you are currently working with and who is under the same guidelines and current precautions as your state leadership mandates. All participants will need to register for the course.
You will need to be able to access Zoom. The instructor will be teaching to all participants via this platform, including live lectures, offering real-time feedback, and answering your questions during lab sessions. Zoom is free to download. Each pair or small group will only need to log in with one device webcam (either laptop or tablet is fine) and will need to have working video and audio in order that the instructor can see you during lab time and hear your questions. Access to the meeting will be password protected and no genitalia will be displayed during the lab sessions.
You will need the following supplies to participate fully:
A treatment table or other solid surface on which a participant can lie during lab time. A hi-low table is ideal but not necessary, a yoga mat on the floor could work in a pinch.
One pillow per participant
One sheet per participant d
Lubricant and wipes
Each participant should bring their own gloves (one set for each lab).
Please treat this like any other live continuing education course. Test your ability to see and hear Zoom (audio and video) prior to the event. Come prepared, having completed the pre-course learning and with all props and supplies already gathered.
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
This is a self-hosted satellite offering of our PF2A course. A satellite course means that the instructor is presently live on Zoom and that participants are gathering in various locations in order to participate and practice labs with one another. Self-hosted means that participants must register in pairs or small groups and practice on each other during lab time.
This continuing education course is comprised of 7 hours and 45 minutes of prerecorded lectures followed by 14 hours of live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
Please note, this is a full lab course that is done remotely. These guidelines represent how we feel you can best experience a remote course. If you feel you are unable to fulfill them then it is recommended that you not participate as a remote learner at this time.
You will need to register with a PT partner. The feedback of your lab partner is highly valuable, therefore you will need to collaborate with another clinician, preferably someone in your clinic or health system that you are currently working with and who is under the same guidelines and current precautions as your state leadership mandates. All participants will need to register for the course.
You will need to be able to access Zoom. The instructor will be teaching to all participants via this platform, including live lectures, offering real-time feedback, and answering your questions during lab sessions. Zoom is free to download. Each pair or small group will only need to log in with one device webcam (either laptop or tablet is fine) and will need to have working video and audio in order that the instructor can see you during lab time and hear your questions. Access to the meeting will be password protected and no genitalia will be displayed during the lab sessions.
You will need the following supplies to participate fully:
A treatment table or other solid surface on which a participant can lie during lab time. A hi-low table is ideal but not necessary, a yoga mat on the floor could work in a pinch.
One pillow per participant
One sheet per participant d
Lubricant and wipes
Each participant should bring their own gloves (one set for each lab).
Please treat this like any other live continuing education course. Test your ability to see and hear Zoom (audio and video) prior to the event. Come prepared, having completed the pre-course learning and with all props and supplies already gathered.
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Start Date/Time and Time Zone:
Feb 11, 2023 7:30 AM America/Phoenix
Location
Venue: Cancer Treatment Centers of America Phoenix
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Level 2A - La Jolla, CA - Dec. 11-13, 2015
{dtregister}265{/dtregister}
{gallery width=181}course_images/pf2a{/gallery}
Description
Schedule
Objectives
Instructor
Location/Lodging
Discounts
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessement (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org 6. Gray's Anatomy for Students - Ebook available at a 20% discount at the preceding link. Use discount code GR56R4W59Q. Registrants who already own a copy, are not required to purchase an additional one. Please Contact Us with any questions about the use of this text as a required reading in this course.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Jenni Gabelsberg, DPT, WCS, MSc, MTC, PRPC
Dr. Jenni Gabelsberg, DPT, MSc, MTC is a women's health physical therapist specializing in urinary incontinence and pelvic pain since 1994. She strives to empower patients through education and self-awareness to encourage them to take responsibility for their own health. She believes that a physical therapist's education forms the cornerstone of her care. She attended the University of Vermont and earned a Bachelor of Science, Physical Therapy, in 1994. She went on to earn a Manual Therapy Certification (MTC) awarded by the Institute of Physical Therapy in 1995. Dr. Gabelsberg next earned an Advanced Masters in Orthopedic Physical Therapy from the University of Saint Augustine for Health Sciences in 1999, and a Doctorate in Physical Therapy in 2003.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location:Click here if map is not shown below.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Start Date/Time and Time Zone:
Nov 12, 2022 8:30 AM America/Chicago
Location
Venue: Ascension SE Wisconsin at Mayfair Road (Wauwatosa)
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessement (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org 6. Gray's Anatomy for Students - Ebook available at a 20% discount at the preceding link. Use discount code GR56R4W59Q. Registrants who already own a copy, are not required to purchase an additional one. Please Contact Us with any questions about the use of this text as a required reading in this course.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Elizabeth Hampton PT, DPT, WCS, PRPC, BCB-PMD
Elizabeth Hampton PT, DPT, WCS, PRPC, BCB-PMD is a Board Certified Women's Health Clinical Specialist in practice since 1987, specializing in pelvic ring dysfunction and movement-education. Elizabeth earned her BS in physical therapy from Marquette University in 1987. She earned her post-bac Certificate in Women's Health Physical Therapy in 2002 and is also a trained childbirth educator and doula. Elizabeth earned the Rehabilitation Certification in Pilates through Polestar Pilates Education in 2003 and integrates the Pilates method into manual therapy and rehabilitation. She earned certification in Pelvic Muscle Dysfunction Biofeedback through the Biofeedback Certification Institute of America in 2005. She has designed and instructed continuing education courses relating to pelvic floor dysfunction and Pilates- based rehabilitation. She is a member of the APTA, the Orthopedic section, the Section on Women's Health as well as the Washington State Physical Therapy Association. Elizabeth is a SACE item writer for the APTA Board Certification Clinical Specialist Exam in Women's Health.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day (8 hours of online content, followed by a 2-day in-person course) intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner was born and raised in Duluth, Minnesota, and has lived in Washington state for most of her adult life. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and in Pelvic Rehabilitation. She teaches continuing education courses nationally, teaches in the transitional Doctor of Physical Therapy program for the College of St. Scholastics, and serves as a consultant for practice and program development. She is a member of the American Physical Therapy Association and the American Massage Therapy Association.
Darla graduated from Louisiana State University (Shreveport, LA) with her physical therapy degree, performed residency training in Women’s Health PT at Duke University, and completed a Ph.D. at the University of Arkansas Medical Sciences. Her dissertation research focused on using non-invasive brain stimulation to augment behavioral interventions for women with lifelong vaginismus, and her ongoing line of research focuses on painful intercourse and post-Cesarean rehabilitation.
Darla’s certifications and training include Women’s Health Certified Specialist (WCS, board certification through the American Board of Physical Therapy Specialties). Certificate of Achievement in Pelvic Physical Therapy (CAPP-Pelvic). Certificate of Achievement in Pregnancy & Postpartum Physical Therapy (CAPP-OB). Certified Lymphedema Therapist (CLT).
Darla began her women’s health physical therapy career in her first job while working with pregnant women with musculoskeletal problems in a private outpatient therapy clinic in Shreveport, LA (with a focus on spine rehab). While there, she developed and hosted an exercise class for pregnant women. She would go on to develop a mom and baby postpartum exercise class while in her Duke residency in Durham, NC. She went on to develop the pelvic, pregnancy, and post-breast cancer/lymphedema PT program at Christus-Schumpert Health System in Shreveport, LA. During this time, she participated in educating women in the labor and birth preparatory classes hosted by the hospital; she also taught the women’s health course for physical therapy students at LSU-Shreveport. Darla went on to serve as a full-time faculty member in the physical therapy program at the University of Central Arkansas in Conway, AR, where she taught women’s health topics, documentation, therapeutic exercise, professional development, and human physiology. She recently owned a private PT practice that is dedicated to pelvic (bowel, bladder, and pelvic pain) and pregnancy/postpartum conditions in Conway, AR. Darla now is a full-time faculty member in the entry-level Physical Therapy program at Graceland University.
Darla currently serves as the President for the Academy of Pelvic Health of the American Physical Therapy Association. She has several peer-reviewed and non-peer-reviewed scientific publications. Amongst some of these, she co-authored “Clinical Summary: Urinary Incontinence” for PTNow.org in April 2015. She authored the chapter titled “The Female Hip and Pelvis” in Orthopedic Management of the Hip and Pelvis (S Cheatham, M Kolber, Elsevier, 2015). She chaired the committee for and participated heavily in the development of the Certificate of Achievement in Pregnancy/Postpartum (CAPP-OB) course series for the Section on Women’s Health of the American Physical Therapy Association. Darla has spoken and instructed many courses in local, national, and international settings on a variety of pelvic, pregnancy/postpartum, and other women’s health physical therapy topics. Darla has served as the Director of Education (2011-2014) and as Vice President (2015-2016) for the Section on Women’s Health, American Physical Therapy Association. She also served a technical expert panel member on Treatments for Fecal Incontinence, Agency for Healthcare Research and Quality in 2014-2015. She also volunteered as a Women’s Health Certified Specialist Exam Standardization Task Force member in May 2013. Darla received several awards from the Section on Women’s Health: CAPP-OB Instructor of the Year (2017); Course Site Hostess of the Year (2018); and Volunteer of the Year (2015). She also received Clinical Instructor of the Year while serving as a clinical instructor a pelvic health physical therapy student from Elon University in 2011.
On a personal note, Darla has teenaged twin boys. She is a lifelong runner and exerciser who loves dark chocolate, craft beer, and her four dogs.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day (8 hours of online content, followed by a 2-day in-person course) intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Stacey Futterman Tauriello, PT, MPT, WCS, BCB-PMD, PPRC, received her Master’s Degree in Physical Therapy from Nova Southeastern University in South Florida in 1996. After graduation she relocated to Chicago where she began specializing in women’s health issues including the treatment of incontinence, pelvic pain and prenatal/postpartum musculoskeletal issues. She returned to the east coast in 2003 and is now the owner of 5 Point Physical Therapy, a specialty physical therapy clinic for male and female pelvic dysfunction in New York City. Stacey, along side Dr. Deborah Coady, recently presented for International Pelvic Pain Society’s annual meeting in Chicago on their research of hip pathology and its relationship to pelvic pain. She has been featured on CBS New York and has presented for the APTA National Conference 2007 for the treatment of male pelvic pain.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a self-hosted satellite offering of our PF2A course. A satellite course means that the instructor is presently live on Zoom and that participants are gathering in various locations in order to participate and practice labs with one another. Self-hosted means that participants must register in pairs or small groups and practice on each other during lab time.
This continuing education course is comprised of 7 hours and 45 minutes of prerecorded lectures followed by 14 hours of live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
Please note, this is a full lab course that is done remotely. These guidelines represent how we feel you can best experience a remote course. If you feel you are unable to fulfill them then it is recommended that you not participate as a remote learner at this time.
You will need to register with a PT partner. The feedback of your lab partner is highly valuable, therefore you will need to collaborate with another clinician, preferably someone in your clinic or health system that you are currently working with and who is under the same guidelines and current precautions as your state leadership mandates. All participants will need to register for the course.
You will need to be able to access Zoom. The instructor will be teaching to all participants via this platform, including live lectures, offering real-time feedback, and answering your questions during lab sessions. Zoom is free to download. Each pair or small group will only need to log in with one device webcam (either laptop or tablet is fine) and will need to have working video and audio in order that the instructor can see you during lab time and hear your questions. Access to the meeting will be password protected and no genitalia will be displayed during the lab sessions.
You will need the following supplies to participate fully:
A treatment table or other solid surface on which a participant can lie during lab time. A hi-low table is ideal but not necessary, a yoga mat on the floor could work in a pinch.
One pillow per participant
One sheet per participant d
Lubricant and wipes
Each participant should bring their own gloves (one set for each lab).
Please treat this like any other live continuing education course. Test your ability to see and hear Zoom (audio and video) prior to the event. Come prepared, having completed the pre-course learning and with all props and supplies already gathered.
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Pelvic Floor Level 2A - Olympia, WA - April 22-24, 2016 (SOLD OUT!)
{dtregister} 333 {/dtregister}
{gallery width=181}course_images/pf2a{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessement (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org 6. Gray's Anatomy for Students - Ebook available at a 20% discount at the preceding link. Use discount code GR56R4W59Q. Registrants who already own a copy, are not required to purchase an additional one. Please Contact Us with any questions about the use of this text as a required reading in this course.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify the muscle layers and specific muscles of the pelvic floor 2. List the pelvic floor muscle functions 3. Describe and perform pelvic floor muscle evaluation techniques utilizing observation, vaginal palpation, and SEMG biofeedback 4. List appropriate outcome measure tools for urinary incontinence, pelvic organ prolapse and pelvic pain 5. List indications, precautions, contraindications, and universal precautions for pelvic floor examination and treatment 6. Identify specific pelvic pain conditions (vulvodynia, IC and CPP) and common physical therapy interventions 7. Identify the various types of urinary incontinence and behavioral treatment options available to the physical therapist 8. List two diagnoses that would benefit from applications of electrotherapy 9. Describe the applications of SEMG biofeedback for the pelvic floor 10. Develop evidence-based treatment plans and progressive clinical goals for female pelvic floor dysfunctions
Attending a remote course is easy and safe, and you can do it entirely from the security and comfort of your own home or clinic without having to find a lab partner.
Important thing to note:
- Our policy for applying for continuing education credit for remote courses differs from that of our in-person and satellite lab courses. Read the specific language of the policy here. Depending on the state in which you practice, you may need to submit your own application to your state board or approving body should you wish that it be approved for continuing education credit in your state.
- To attend a remote Herman & Wallace course, registrants will need Zoom video conferencing software. This is a requirement. One can create an account and download the software to their computer at https://zoom.us/
- We use the Pacific Time Zone for all of our remote course start and end times (this is not the case for in-person and satellite lab locations). Please make a note of this and set your calendar accordingly.
- A Zoom account is free to create. Before the meeting, we recommend having a practice Zoom session with a friend or colleague so you can test your microphone, video, and internet connection. You can participate in any remote course from the comfort of your home, but will need a stable internet connection in order to participate. We recommend downloading the software and practicing a call with a friend or colleague prior to your course with us. Zoom also offers video tutorials on their website at https://support.zoom.us/hc/en-us/articles/206618765-Zoom-Video-Tutorials.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Pelvic Floor Level 2A - San Diego, CA - December 1-3, 2017 (SOLD OUT)
{dtregister}512{/dtregister}
{gallery width=181}course_images/pf2a{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price: $695 ($725 within one month of the course) Experience Level: Intermediate Contact Hours: 22.5
This continuing education course is a three-day (8 hours of online content, followed by a 2-day in-person course) intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect quality of life so dramatically. In the US, adult estimates of fecal incontinence is over 8%, and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included on Day 2 of this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. Day 3 of the course introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Special Considerations:
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. Teachable is where you will find pre-recorded videos and other pre-requisite learning, manual files, your liability waiver you must sign in order to participate, and any links to Zoom (if the course is a remote option). After the course is over, Teachable is where you will find your post-test and evaluation form to tell us what you thought, as well as your certificate. It is required in Teachable that you complete all components in order. Pre-recorded videos that are required must be watched before going onto the next session.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
Recorded Lecture: Watch Before the In-Person Component of the Course
7:30 Registration 8:00 Introduction, Goals, Objectives 8:30 Colorectal Anatomy and Physiology Review, Anorectal Examination 9:15 LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 10:15 Break 10:30 Fecal Incontinence, Case Study 11:15 Constipation, Case Study 12:00 Lunch 1:00 Pelvic Pain: Prostatitis, Scrotal Pain 2:00 Coccyx Dysfunction 3:00 Break 3:15 LAB 2: External Palpation & Intervention Posterior Pelvis 4:15 Prostatectomy Part I 5:15 Questions 5:30 Adjourn
Day Two:
7:45 Questions from Day 1, Post-test Day 1 8:00 Prostatectomy Part II 8:45 Pudendal 9:45 Break 10:00 LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 11:15 LAB 4: Inclusive Language 12:00 Lunch 12:45 Colorectal Conditions 2:00 Break 2:15 LAB 5: Final Pelvic Rehabilitation Examination, Evaluation, & Treatment 3:30 Questions 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Jessica Reale, PT, DPT, WCS
Jessica is a board-certified specialist in Women’s Health (WCS) and is passionate about working with all people with pelvic floor disorders, especially those with chronic pelvic pain, urinary dysfunction and bowel dysfunction. She is a graduate of Gordon College with a B.S. in Kinesiology and of Duke University where she received her Doctor of Physical Therapy degree. Jessica owns and treats patients at Southern Pelvic Health in Atlanta, GA, a specialty pelvic rehabilitation practice.
Jessica is passionate about pelvic health education, and works closely with Holly Tanner in writing and updating Pelvic Floor Level 1, 2A and 2B coursework. She also regularly guest lectures at local university DPT programs, and has presented at conferences, seminars, community groups, and various medical and physical therapy residency programs.
Jessica loves supporting other pelvic rehabilitation providers, and founded the Facebook group, Pelvic PT Newbies, as a place for safe questioning, learning and growth. She also established and runs a professional small group mentoring program several times each year. She also runs an educational blog on pelvic health topics through her website, and is active on social media @southernpelvichealth, spreading awareness of pelvic floor dysfunction and pelvic rehabilitation. Outside of work, Jessica enjoys spending time with her husband and 2 daughters, staying active, and traveling. .
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location:click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
</>This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Start Date/Time and Time Zone:
Nov 12, 2022 9:30 AM America/New_York
Location
Venue: Ivy Rehab (Charlottesville, VA)
Address:
1460 Pantops Mountain Place
Suite 203
Charlottesville VA 22911
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a self-hosted satellite offering of our PF2A course. A satellite course means that the instructor is presently live on Zoom and that participants are gathering in various locations in order to participate and practice labs with one another. Self-hosted means that participants must register in pairs or small groups and practice on each other during lab time.
This continuing education course is comprised of 7 hours and 45 minutes of prerecorded lectures followed by 14 hours of live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient.Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations:
Please note, this is a full lab course that is done remotely. These guidelines represent how we feel you can best experience a remote course. If you feel you are unable to fulfill them then it is recommended that you not participate as a remote learner at this time.
You will need to register with a PT partner. The feedback of your lab partner is highly valuable, therefore you will need to collaborate with another clinician, preferably someone in your clinic or health system that you are currently working with and who is under the same guidelines and current precautions as your state leadership mandates. All participants will need to register for the course.
You will need to be able to access Zoom. The instructor will be teaching to all participants via this platform, including live lectures, offering real-time feedback, and answering your questions during lab sessions. Zoom is free to download. Each pair or small group will only need to log in with one device webcam (either laptop or tablet is fine) and will need to have working video and audio in order that the instructor can see you during lab time and hear your questions. Access to the meeting will be password protected and no genitalia will be displayed during the lab sessions.
You will need the following supplies to participate fully:
A treatment table or other solid surface on which a participant can lie during lab time. A hi-low table is ideal but not necessary, a yoga mat on the floor could work in a pinch.
One pillow per participant
One sheet per participant d
Lubricant and wipes
Each participant should bring their own gloves (one set for each lab).
Please treat this like any other live continuing education course. Test your ability to see and hear Zoom (audio and video) prior to the event. Come prepared, having completed the pre-course learning and with all props and supplies already gathered.
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Rectal pelvic floor muscle examinations will be taught in labs. Past participants have found that wearing comfortable clothing that is easy for changing (such as skirts or athletic shorts) is very useful for labs. Due to temperature variations from clinic to clinic we would recommend wearing comfortable layers.
PLEASE NOTE: This course includes internal assessment and exam techniques, which will be practiced in partnered pairs in lab time. H&W strives to foster an environment that is safe and supportive. Survivors of past trauma should be aware that performing or experiencing internal exam may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Required Readings:
1. The National Digestive Diseases Information Clearinghouse Handout on Fecal Incontinence 2. The National Institute of Diabetes and Digestive and Kidney Diseases Article on Constipation 3. The International Pelvic Pain Society Article on Pudendal Nerve Entrapment (PNE) 4. The European Urology Association'sGuidelines on Chronic Pelvic Pain 5. Principles of Biofeedback from Professor Tim Watson's website electrotherapy.org
6. Gray's Anatomy for Students - Available at a 25% Discount for Herman & Wallace registrants with promo code 70484. Registrants who already own a copy of this or a corresponding textbook are not required to purchase an additional one.
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2A)
Course Description
This is a satellite offering of our course, Pelvic Floor Level 2A. This continuing education course consists of 9.3 hours of pre recorded lectures followed by 13.75 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self-hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
PLEASE NOTE: This location requires that participants bring their own laptop and headphones to each course hosted here. Attendees will participate from treatment rooms in the facility, and will be joining the course Zoom from their personal laptops.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
PLEASE NOTE: This location requires that participants bring their own laptop and headphones to each course hosted here. Attendees will participate from treatment rooms in the facility, and will be joining the course Zoom from their personal laptops.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course, Pelvic Floor Level 2A. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This continuing education course is comprised of prerecorded lectures followed by live, interactive remote learning and is an intermediate-level seminar designed as a next step in completing the clinicians’ ability to more comprehensively evaluate and treat the female and male pelvic floor. The participant will have the opportunity to learn about two common bowel dysfunctions, fecal incontinence and constipation, and how the pelvic rehabilitation provider can play a crucial role in overcoming these issues that affect the quality of life so dramatically. In the US, the estimate of adult fecal incontinence is over 8% and greater than 15% in people over age 70. (Whitehead, 2010) According to the National Institutes of Health, constipation affects up to 15% of people, and is one of the most common gastrointestinal complaints that affects 42 million people. (Constipation, 2013) Pelvic rehabilitation providers are able to teach patients how to significantly improve quality of life through simple behavioral techniques and approaches that optimize abdominopelvic health.
Participants will learn how to evaluate the patient who presents with bowel dysfunction including fecal incontinence and constipation, and also with defecation disorders such as paroxysmal puborectalis, irritable bowel syndrome (IBS), and fecal urgency. Knowledge of pelvic anatomy expands into the gastrointestinal system with detailed instruction about the rectum and anal canal, anal sphincters, and with instruction in important physiologic principles such as the gastrocolic reflex, sampling response, and intrinsic defecation reflex. There are other conditions that can cause pain or bleeding such as hemorrhoids, fistulas, fissures, and proctalgia fugax; the clinician will learn how to apply skills of external and internal pelvic muscle assessment (via the anorectal canal) for these conditions.
Many pelvic rehabilitation providers attend this course to learn clinical skills for coccyx pain and for pudendal neuralgia, two conditions that are included in this continuing education course. As either condition can contribute to chronic pelvic pain, this course provides significant lab time so that participants will have the opportunity to practice any new skills. The course also introduces the participant to pelvic rehabilitation of the male patient with an emphasis on topics of male pelvic anatomy, urinary incontinence, prostatectomy, and male pelvic pain. The content in this course prepares the therapist to work with male pelvic conditions by reinforcing what is common to the care of both men and women, as well as teaching that which is unique for the male patient. Current medical evaluation (with tests such as defecography, manometry), medical management (for anorectal pain and for colorectal conditions), and evidence-informed clinical interventions will be instructed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Anorectal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
Constipation. (2013) National Institutes of Health. Retrieved January 22, 2014 from http://digestive.niddk.nih.gov/ddiseases/pubs/constipation Whitehead, W. E., Borrud, L., Gode, P. S., Meikle, S., Mueller, E. R., Tuteja, A.,...Ye, W. (2009). Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology, (137)2, 512-517
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction, Goals, Objectives
6:50 - Colorectal Anatomy and Physiology Review, Anorectal Examination Lab Prep 7:45 - LAB 1: Anorectal Evaluation: Sidelying Anorectal Examination & Muscle Mapping 8:45 - Break 9:00 - Fecal Incontinence, Case Study 9:45 - Constipation, Case Study 10:45 - Lunch 11:45 - Pelvic Pain: Prostatitis, Scrotal Pain & Spermatic Cord 12:45 - Coccyx Dysfunction 1:45 - Break 2:00 - LAB 2: External Palpation & Intervention Posterior Pelvis 3:00 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Prostate & Prostatectomy Part II - Rehabilitation 7:45 - Pudendal Nerve Dysfunction Part II 8:30 - Break 8:45 - Pudendal Nerve Dysfunction Part II (Continued) 9:15 - LAB 3: Internal Interventions for Coccyx, Pudendal and Pelvic Pain 10:45 - Lunch 11:30 - LAB 4: Inclusive Language 12:15 - Break 12:30 - Colorectal Conditions 2:00 - Questions 2:15 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Describe anatomy of the colorectal region. 2. Explain physiology of the gastrointestinal system including pathophysiology pertaining to bowel dysfunction. 3. Perform examination and evaluation of pelvic floor function related to anorectal structures. 4. Recognize types of fecal incontinence and develop plans of care for intervention including behavioral training and education. 5. Recognize and treat constipation, name the signs, symptoms, and interventions for hemorrhoids, fissures, fistulas, and other common colorectal conditions. 6. Identify specific pelvic floor muscles and key bony landmarks within the anorectal canal. 7. Perform external and internal rectal myofascial treatment techniques such as Thiele’s massage and trigger point release. 8. Perform patient education and behavioral training for constipation, fecal incontinence and pelvic pain syndromes. 9. Describe and teach three SEMG downtraining (relaxation) strategies for the overactive pelvic floor. 10. Describe and demonstrate coccyx evaluation and treatment using internal and external coccyx mobilizations. 11. Describe male urogenital and pelvic floor anatomy, identify signs and symptoms of prostatodynia 12. List key medical diagnostic procedures for colorectal conditions.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Practical, trauma aware, hands-on labs will include an external abdominal and pelvic and internal vaginal approach. Labs will focus on pelvic structures in relationship to the vaginal canal and surrounding structures such as the lumbopelvic nerves, the uterus, urethra, bladder, and rectum. Interventions instructed will include patient management of trunk and pelvic pressure, relaxation training, breathing, and manual therapies for a variety of pelvic dysfunctions. The information contained in this course is immediately applicable to clinical practice.
For pelvic conditions, the clinician will learn to: -- Recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities for specific conditions -- Use an evaluation/outcome tool appropriate to the patient’s concerns -- Design a multi-modal plan of care for pelvic rehabilitation -- Perform clinical interventions based on the patient’s needs and goals
Clinical treatment interventions will include patient education, neuro re-education, therapeutic exercisemanual therapy, therapeutic activities, instruction in self-care, and recommendations for relevant modalities
Prerequisites Our course Pelvic Function Level 1 or Pelvic PT 1 through the APTA, is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Pre-Course Learning Requirements 10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. In Teachable, registrants will find recorded video lectures (all recorded video lectures must be completed before attending the first day of class), other pre-requisite learning materials, course manual files, mandatory liability waiver, and URLs for any Zoom meetings. We require registrants to complete teachable components in sequential order. Videos lectures are required and must be completed in-full before proceeding to the next Teachable section. At the conclusion of the course, registrants can access their post-test and course evaluation form to provide our curriculum team feedback on their experience, as well as download their certificate of completion - all via Teachable.
Audience This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Read more aboutWhat to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
<p
Jenni Gabelsberg, DPT, WCS, MSc, MTC, PRPC
Dr. Jenni Gabelsberg, DPT, MSc, MTC is a women's health physical therapist specializing in urinary incontinence and pelvic pain since 1994. She strives to empower patients through education and self-awareness to encourage them to take responsibility for their own health. She believes that a physical therapist's education forms the cornerstone of her care. She attended the University of Vermont and earned a Bachelor of Science, Physical Therapy, in 1994. She went on to earn a Manual Therapy Certification (MTC) awarded by the Institute of Physical Therapy in 1995. Dr. Gabelsberg next earned an Advanced Masters in Orthopedic Physical Therapy from the University of Saint Augustine for Health Sciences in 1999, and a Doctorate in Physical Therapy in 2003.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Pelvic Floor Level 2B - Kirkland, WA - February 26-28, 2016 (SOLD OUT!)
{dtregister}366{/dtregister}
{gallery width=181}course_images/pf2b{/gallery}
Description
Schedule
Objectives
Instructors
Location/Lodging
Discounts
Price: $695 (Early Registrant Price of $675 ends one month before the first day of the course). Note pricing changes for 2017 courses Experience Level: Intermediate Contact Hours: 22.5
This three day intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including downtraining of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. . Evidence-based references and case studies will be presented for thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have two instructors and several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points is instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and to care of the patient is discussed.
Please note, the Pelvic Floor series of courses typically fill up about 2-3 months before the scheduled course date. It is highly recommended that participants register well in advance to reserve their seats. If you need your employer to send a check for your registration payment, please click the Request Invoice button on the course event page to reserve your seat.
Special Considerations: As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
The Herman & Wallace Institute welcomes all professionals who are appropriately licensed at our courses. Being born with a vagina and other female anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other one participant during labs.
Pregnant women course attendees may participate fully in the entire course if they bring their own lab model for examination, or if the attendee insists on lab participation then a clearance letter from their physician allowing them to participate in the labs is required. We strongly recommend that pregnant attendees bring a model as vaginal examination and internal myofascial manual therapy prior to 32 weeks gestation is not the common standard of medical practice. If pregnant participants cannot bring a model, they have the option of working in a group of three during lab times.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Assignments:
In order to derive the most benefit from this course, we ask our participants to internalize the required reading materials and complete a diary assignment prior to attending. Please complete this assignment prior to the first day of the seminar.
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Tina Allen, PT, PRPC, BCB-PMD
Tina Allen, PT, PRPC, BCB-PMD has been a physical therapist since 1993. She received her PT degree from the University of Illinois at Chicago. Her initial five years in practice focused on acute care, trauma, and outpatient orthopedic physical therapy at Loyola Medical Center in Illinois. Tina moved to Seattle in 1997 and focused her practice in Pelvic Health. Since then she has focused her treatment on the care of all genders throughout their life spans with bladder/bowel dysfunction, pelvic pain syndromes, pregnancy/ postpartum, lymphedema, and cancer recovery.
Tina’s practice is at the University of Washington Medical Center in the Urology/Urogynecology Clinic where she treats along side physicians and educates medical residents in how pelvic rehab interventions will assist clients. She presents at medical and patient conferences on topics such as pelvic pain, continence, and lymphedema. Tina has been faculty at Herman and Wallace Pelvic Rehabilitation Institute since 2006. She was the physical therapist provider for the University of Washington on a LURN Multi-Center study for Interstitial Cystitis/Painful Bladder Syndrome treatment with physical therapy techniques. Tina was also a co-investigator for a content package on pain education for the NIDA/NIH on treatment of pelvic pain.
Outside work Tina enjoys spending time with her husband, hiking, traveling, reading and meditation.
Directions from Recommended Lodging to Course Location
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Pelvic Floor Level 2B - Maywood, IL - May 29-31, 2020 (Rescheduled)
Update 4/17/2020: As a precaution against the spread of COVID-19, this course has been postponed. Once we have a new date confirmed, we will update our website and make the event available for registration. We appreciate your understanding during this difficult time. Please practice good hygiene, and be safe!
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Practical, trauma aware, hands-on labs will include an external abdominal and pelvic and internal vaginal approach. Labs will focus on pelvic structures in relationship to the vaginal canal and surrounding structures such as the lumbopelvic nerves, the uterus, urethra, bladder, and rectum. Interventions instructed will include patient management of trunk and pelvic pressure, relaxation training, breathing, and manual therapies for a variety of pelvic dysfunctions. The information contained in this course is immediately applicable to clinical practice.
For pelvic conditions, the clinician will learn to: -- Recognize the key signs and symptoms that lead to impairment, functional limitations and disabilities for specific conditions -- Use an evaluation/outcome tool appropriate to the patient’s concerns -- Design a multi-modal plan of care for pelvic rehabilitation -- Perform clinical interventions based on the patient’s needs and goals
Clinical treatment interventions will include patient education, neuro re-education, therapeutic exercisemanual therapy, therapeutic activities, instruction in self-care, and recommendations for relevant modalities
Prerequisites Our course Pelvic Function Level 1 or Pelvic PT 1 through the APTA, is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
Pre-Course Learning Requirements 10-14 days before the course, participants will receive an invite to join Teachable, an online learning platform. In Teachable, registrants will find recorded video lectures (all recorded video lectures must be completed before attending the first day of class), other pre-requisite learning materials, course manual files, mandatory liability waiver, and URLs for any Zoom meetings. We require registrants to complete teachable components in sequential order. Videos lectures are required and must be completed in-full before proceeding to the next Teachable section. At the conclusion of the course, registrants can access their post-test and course evaluation form to provide our curriculum team feedback on their experience, as well as download their certificate of completion - all via Teachable.
Audience This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Read more aboutWhat to Expect During Courses with Internal Lab Work.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner was born and raised in Duluth, Minnesota, and has lived in Washington state for most of her adult life. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and in Pelvic Rehabilitation. She teaches continuing education courses nationally, teaches in the transitional Doctor of Physical Therapy program for the College of St. Scholastics, and serves as a consultant for practice and program development. She is a member of the American Physical Therapy Association and the American Massage Therapy Association.
Originally from the heart of Packer country in Eastern Wisconsin, Meghan graduated from The College of St Scholastica in Duluth, MN in 2000 with her Master of Arts in Physical Therapy and relocated to the Twin Cities area. Initially, an orthopedic therapist, Meghan wanted nothing to do with pelvic health, nor knew much about it! After the birth of her own children, she developed pelvic pain and was on a quest to find a path of healing for herself and realized what a profound impact her pelvic health therapist had on getting her life back! These experiences opened her up to a whole new passion and dedication she never imagined that would also have such an impact on the patients she serves. She has been an advocate for pelvic health for both women and men over the past several years.
Meghan has presented to several community groups, doctors’ groups, as well as other therapists on pelvic health treatment, differential diagnosis, and chronic pelvic pain. Additionally, she serves as a clinical instructor for DPT students.
Meghan believes in educating and empowering patients to get better, live a more active and healthier lifestyle, and to educate all on the importance of pelvic health.
Meghan currently practices, is a Clinic Supervisor and Clinical Specialist at The Institute for Athletic Medicine in Lino Lakes and Hugo, MN. She primarily treats women and men with chronic pelvic pain, incontinence, and constipation.
In her spare time, she enjoys spending time with her husband, 3 kids, 2 dogs, camping, hiking, watching the Green Bay Packers and is a member of her children’s soccer board!
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Start Date/Time and Time Zone:
Jan 28, 2023 6:30 AM America/Los_Angeles
Location
Venue: Life in Balance Physical Therapy - Normandy Park Office
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Destiny Bochinski, PT, DPT, PRPC (Encinitas, CA)
Destiny is originally from Oregon but relocated to southern California after earning her Bachelor’s in Biology from Linfield College, where she also minored in Theatre Arts. She then went on to earn her Doctor of Physical Therapy from Chapman University in 2008. She developed a passionate interest in pelvic health when she attended the midwife-assisted home births of her two nephews. Since then, she has enjoyed educating patients, colleagues, physicians, nurses, and the community through in-services, classes, and podcasts delivered in a variety of venues. She is thrilled to be part of the faculty at Herman & Wallace, teaching the pelvic floor series continuing education courses.
Destiny treats men and women with urinary, gynecologic, colorectal, and orthopedic dysfunctions as the lead pelvic health physical therapist at a hospital-based outpatient clinic in Encinitas, California. She believes her primary role is as an educator for her patients to empower them to become advocates for their own health and active participants in their rehabilitation.
Outside of work, Destiny enjoys spending time with her 2 children and husband, hiking, swimming, yoga, and tasting wine.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of pre recorded lectures followed by live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of 8 hours of pre recorded lectures followed by 14.5 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This three-day (8 hours of online content, plus 2-days of in-person learning) intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of 8 hours of pre recorded lectures followed by 14.5 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This three-day (8 hours of online content, plus 2-days of in-person learning) intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Floor Function, Dysfunction and Treatment (Level 2B)
Course Description
This is a satellite offering of our course Pelvic Floor Level 2B. This continuing education course consists of 8 hours of pre recorded lectures followed by 14.5 hours of live, interactive remote learning which will be completed by groups meeting at a specific satellite location OR self hosted location. The instructor will be presenting to all satellites from a remote location via Zoom. During labs, participants will pair up and be guided by the local lab assistants at the satellite course location.
This three-day (8 hours of online content, plus 2-days of in-person learning) intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
This is a "self-hosted" option for attending a satellite lab course. Registrants who would like to pursue this option must:
Locate another therapist or small group of therapists who would like to register together as a unit. Individual registrations without a qualified and registered partner are not permitted.
Find a suitable location from which the pair/group can all view the zoom lectures together.
Practice hands-on lab techniques on the other therapists in their pair/group without a lab assistant or instructor physically present at their self-hosted location. The instructor will provide remote direction via zoom.
Students are required to attend a hosted satellite course option and are not permitted to register for self-hosted events.
Those who wish to take this course, but cannot meet the above requirements should register for a satellite location or in-person version of this course
What to have on hand for self-hosted labs
Your partner! You will need at least one person to work with during labs. This person must be a licensed professional who is also registered for the course. The printable portion of your manual from Teachable if you choose to print. * You are not required to print your full manual, please check for any sections specifically asking you to print prior to the event. Your Mask- Please wear a mask while participating in this course to keep your colleagues safe. A computer with a Wifi connection that your group will be using to view the course. The following supplies: Non Latex, Non-Powder Vinyl Gloves MEDIUM (box of 100) Hand Sanitizer (8 fl. Oz.) Lube for labs
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
This is a satellite offering of our course Pelvic Floor Level 2B. A satellite means that participants will be gathering in a given location and watching the instructor present remotely on the same screen. During labs, participants at the satellite course locations will pair up and be guided by the local lab assistants. Self Hosted pairs and groups will not be provided a lab assistant and will instead be guided remotely by the course instructor..
This intermediate-level continuing education course further defines skills and knowledge learned in the foundational Pelvic Floor Level One course. Specific, advanced examination techniques such as pelvic muscle mapping and interventions including down training of overactive muscles is instructed. With a specific focus on urogynecologic conditions including prolapse and pelvic organ descent, various pelvic pain diagnoses, and abdominal wall rehabilitation, the participant will be able to learn specific skills to treat these conditions that have a significant negative impact on a woman's health. Evidence-based references and case studies will be presented for a thorough understanding of current medical evaluation and management of each condition.
Instruction in female urogynecologic anatomy occurs throughout this continuing education course, along with education in current terminology and clinical models related to the trunk and pelvic control. Detailed internal vaginal and external perineal examinations are included in the practical lab activities, during which the participant will have several experienced lab assistants as guides. An entire lecture is dedicated to the management of prolapse and pelvic organ descent so that the pelvic rehabilitation provider will be able to develop clinical and home program strategies for the patient who presents with conditions such as rectocele, cystocele, or uterine prolapse.
Common conditions associated with female pelvic pain are included throughout the three days of education. Such diagnoses may include vulvar pain, vestibulitis, interstitial cystitis or bladder pain syndrome, episiotomy, dyspareunia, lichen sclerosis, lichen simplex, or lichen planus. Both abdominal and pelvic muscle tenderness is higher in patients who have chronic pelvic pain, and increased pelvic muscle tender points have been noted to correlate with higher rates of depression, dyspareunia (pain with sexual function), and bowel dysfunction. (Montenegro et al., 2009; Montenegro et al., 2010) Assessment and treatment of pelvic and abdominal wall tender points are instructed along with abdominopelvic nerve dysfunction and relaxation training- all are strategies that the clinician can employ immediately following completion of this continuing education course. The important and sensitive topic of sexual abuse and trauma as it relates to pelvic dysfunction and the care of the patient is discussed.
Prerequisites:
Pelvic Floor Level 1, through Herman & Wallace or Pelvic PT 1 through the APTA is required. Exceptions to this policy may be granted on a case-by-case basis, to inquire about such exceptions please contact us.
All pre-recorded lectures in Teachable for this course must be watched before the Live Component of the course and in order to earn a certificate of completion for this course. See the Schedule tab for the current list of pre-recorded videos
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Special Considerations
As this continuing education course includes extensive lab work, all course attendees should come prepared to participate as both clinician and patient. Vaginal pelvic floor muscle examinations will be taught in labs. Labs will be conducted under the supervision of instructors and teaching assistants. There will be a ratio of at least one instructor/assistant for every ten participants.
Participation in Labs
H&W strives to foster an environment that is inclusive and welcomes all professionals who are appropriately licensed at our courses. Having any particular anatomy is not a prerequisite for attending or participating fully in our courses. No one participant will be required to partner with any other participant during labs. Survivors of past trauma should be aware that performing or experiencing internal exams may be triggering, and that many, regardless of their histories, feel strong emotions when practicing these techniques. In order to foster an environment that is non-triggering and safe for all participants, we recommend all participants consider the emotional impact they may experience during the course, and consider consulting a trauma counselor or therapist prior to attending. Read more about What to Expect During Courses with Internal Lab Work.
References
De Souza Montenegro, M. L. L., Mateus-Vasconcelos, E. C. L., Silva, J. C. R. E, Nogueira, A. A., Dos Reis, F. J. C.,& Poli Neto, O. B. (2010). Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain Medicine, 11(2), 224-228. Montenegro, M. L. L. S., Gomide, L. B., Mateus-Vasconcelos, E. L., Rosa-e-Silva, J. C., Candido-dos-Reis, F. J., Nogueira, A. A., & Poli-Neto, O. B. (2009). Abdominal myofascial pain syndrome must be considered in the differential diagnosis of chronic pelvic pain. European Journal of Obstetrics & Gynecology and Reproductive Biology, 147(1), 21-24.
============================= Before Day One
=============================
These video lectures in Teachable must be viewed in-full prior to the course Total video lecture time: 7 hours
1) Pelvic Rehab Concepts, Anatomy, & Specific Palpation (37 min) 2) Trauma-informed Care (55 min) 3) Prolapse (41 min) 4) Medical and Multidisciplinary Management of Pelvic Pain (38 min) 5) Specific Conditions: Vulvar Pain, Dyspareunia, Vaginismus (45 min) 6) Specific Conditions: Interstitial Cystitis/Painful Bladder Syndrome, UTI (43 minutes) 7) Specific Conditions: Endometriosis, PCOS (61 min) 8) Neuromuscular Relaxation Training (39 min) 9) Abdominal Neuromyofascial Anatomy (39 min) 10) Breathing and Pressure Management (31 min)
============================= Day One
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Introduction to abdominopelvic pain and urogynecologic conditions, goals & objectives
7:00 - Abdominopelvic pain and anatomical mapping 8:00 - Lab 1 Prep: Internal vaginal layer palpation and prolapse assessment 8:30 - Break 8:45 - LAB 1: Internal vaginal layer palpation and prolapse assessment 10:15 - Lab synthesis discussion 10:30 - Lunch/Meal Break 11:30 - Prolapse, recovery, and pessary referrals 12:15 - Lab 2 Prep: Breathing & Trunk Mobility, Stability 12:50 - LAB 2: Breathing & Trunk Mobility, Stability 1:30 - Break 1:45 - Vulvar skin conditions and topical medications 2:30 - Case Discussions Part I 3:30 - Adjourn
============================= Day Two
=============================
6:00 am PST - Zoom opens 30 mins before course for registration and setup 6:30 am PST - Course begins / Questions from Day 1 6:45 - Lab 3 Prep: Abdominal neuromyofascial techniques 7:15 - LAB 3: Abdominal neuromyofascial techniques 8:30 - Break 8:45 - Lab 5 Prep: Abdominopelvic and Internal Vaginal Interventions 9:30 - Lab 4: Relaxation techniques 10:30 - Lunch/Meal Break 11:15 - Lab 5: Abdominopelvic and Internal Vaginal Interventions 12:45 - Case Discussions Part II 1:45 - Course Synthesis Discussion 2:00 - Adjourn
Upon completion of this continuing education seminar, participants will be able to:
1. Identify anatomy, physiology, and pathophysiology of the urogynecologic systems with reference to specific vulvovaginal conditions, pelvic organ prolapse (POP), interstitial cystitis/painful bladder syndrome (IC/PBS), and urinary tract infections (UTIs), and polycystic ovarian syndrome (PCOS), and endometriosis
2. Perform detailed and specific pelvic anatomy mapping related to external and internal vulvovaginal conditions
3. Incorporate informed consent, trauma-informed care and an approach that is sensitive to culture and religious beliefs for evaluation and intervention skills.
4. Describe 3 theories of neuromuscular relaxation and how to perform guided relaxation techniques
5. Describe necessity of medical referral and screening as appropriate for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
6. Describe common medical testing, common medical procedures, and multidisciplinary care for vulvovaginal conditions, POP, IC/PBS, and UTIs, PCOS, and endometriosis
7. Perform examination, evaluation, and develop plan of care appropriate for pelvic dysfunctions including vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
8. Recognize signs, symptoms, and rehabilitation interventions for common colorectal conditions such as vaginismus, vulvodynia, dyspareunia, POP, PCOS, IC/PBS, UTI, and endometriosis
9. Identify patient selection criteria for pessary and identify the role of the rehabilitation provider in pessary fitting
10. Describe and demonstrate abdominal wall evaluation and treatment interventions of manual therapy, and specific therapeutic exercise for transversus abdominis, diastasis recti, nerve dysfunction, and myofascial pain
11. Perform internal vaginal myofascial and soft tissue treatment techniques to the pelvic floor and pelvic wall muscles
12. Recognize need for medical consultation for vulvar skin conditions including but not limited to vaginal atrophy, disease conditions, lesions, abnormal coloring and texture, genitourinary syndrome of menopause (GSM)
PLEASE NOTE: This location requires that participants bring their own laptop and headphones to each course hosted here. Attendees will participate from treatment rooms in the facility, and will be joining the course Zoom from their personal laptops.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Pelvic Function Level 2C: Men’s Pelvic Health & Rehabilitation
Course Description
PF2C, Men’s Pelvic Health & Rehabilitation, was born out of the former “Male Pelvic Floor” course to fill the need of providing detailed information for providers interested in working with men’s pelvic health conditions. PF2C is created for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
Start Date/Time and Time Zone:
Jan 20, 2024 6:30 AM America/Los_Angeles
Location
Venue: Rod Lee Bigelow Building of Health Sciences
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
Start Date/Time and Time Zone:
Jan 20, 2024 6:30 AM America/Los_Angeles
Location
Venue: Life in Balance Physical Therapy and Pilates
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
This first course in our Pelvic Function Series, Pelvic Function Level 1 or PF1, is designed to provide a thorough introduction to pelvic health, pelvic dysfunction, and interventions for rehabilitation. We created PF1 for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), pelvic neuralgias, vulvar pain, and dyspareunia may be improved with pelvic rehabilitation. Practical, supervised, hands-on labs will include an external perineal and anorectal approach and internal vaginal examination. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2B (PF2B) is an intermediate-level course which covers increased specificity of evaluation for urogynecologic conditions as well as an overview of medical management, and multi-disciplinary pelvic healthcare. This course is intended for the pelvic health clinician who treats patients with conditions including urinary incontinence, chronic pelvic pain (CPP), and pelvic organ prolapse. Participants will understand how diagnoses such as interstitial cystitis/painful bladder syndrome (IC/PBS), urinary tract infections, vaginismus, vulvar pain, dyspareunia, polycystic ovarian syndrome (PCOS), and endometriosis may be improved with pelvic rehabilitation. This course was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Course Start Date/Time and Time Zone:
Apr 20, 2024 9:30 AM America/New_York
Location
Venue: Hendricks Regional Health - Plainfield Medical Center
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Start Date/Time and Time Zone:
Sep 21, 2024 6:30 AM America/Los_Angeles
Location
Venue: Life in Balance Physical Therapy and Pilates
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
Pelvic Function Level 2C - Men’s Pelvic Health and Rehabilitation (PF2C) is an intermediate-level course designed to provide critical detailed information to providers interested in working with men and men’s pelvic health conditions. This course is intended for the pelvic health clinician who treats patients with conditions including post-prostatectomy urinary incontinence, erectile dysfunction, and chronic pelvic pain (CPP). Participants will understand how diagnoses such as hard/flaccid, urgency/frequency, scrotal, testicular, and penile pain may be improved with pelvic rehabilitation. Practical, hands-on labs will include an external abdominal, gluteal, perineal and internal anorectal approach. The information contained in this course is immediately applicable to clinical practice. This course was born out of the former “Male Pelvic Floor” and was designed as a progression of knowledge and skills learned in the foundational course of our Pelvic Function Series: Pelvic Function Level 1: Introduction to Pelvic Health. The information contained in this course is immediately applicable to clinical practice.
This unique continuing education course addresses topics pertaining to patients during the peripartum period that both the new and the experienced therapist can enjoy. The course begins with a review of labor and delivery, fetal positions and presentations, labor augmentation and induction, and physical therapy in labor. The 2-day course progresses through many areas of "special topics" including conditions that affect fertility such as polycystic ovarian syndrome, endometriosis, thyroidectomies, and a history of cancer. While Caring for Pregnant Patient and Caring for the Postpartum Patient covered many of the common musculoskeletal issues encountered in the peripartum period, this 3rd continuing education course in the Peripartum Series offers more information about connective tissues such as myofascial restrictions and nerve dysfunctions. Gynecologic surgeries and pelvic rehabilitation for the following are included: tubal ligation, vaginal rejuvination, female genital cosmetic surgery, symphysiotomy, and postpartum hysterectomy.
Therapists who are familiar with the evaluation and treatment of women in the peripartum period may find the instruction of caring for special patient populations helpful in clinical practice. Patients who have medical conditions such as spinal cord injury, cystic fibrosis, multiple sclerosis, and lupus face added challenges during pregnancy and postpartum; this continuing education course looks to the research to guide participants' critical thinking towards clinical practice. Components of cultural competence are instructed that include cultural awareness and sensitivity, competent communication between those of differing cultural backgrounds, and cultural beliefs in pregnancy and childbearing practices.
In peripartum, a significant number of women are victims of domestic violence, many times committed by an intimate partner. (Daoud et al., 2012) The US Department of Health and Human Services recommends that intimate partner violence screening should occur as a core part of women's health care; participants will learn about the negative maternal and fetal health impact of abuse and will learn screening and reporting methods as well. Participants will have the opportunity to share a brief exercise "assignment" that is completed prior to attending the course, with assignments also presented by colleagues. There is timed carved out in the schedule to ask the instructor about any peripartum question such as a patient case-related issue, program development, or general treatment of the peripartum patient.
Audience:
This continuing education seminar is targeted to physical therapists, occupational therapists, physical therapist assistants, occupational therapist assistants, registered nurses, nurse midwives, and other rehabilitation professionals. Content is not intended for use outside the scope of the learner's license or regulation. Physical therapy continuing education courses should not be taken by individuals who are not licensed or otherwise regulated, except, as they are involved in a specific plan of care.
Prerequisites:
It is recommended that the participant have experience and at least one course in pregnancy and post-partum issues prior to taking this “special topics” course.
Assignments:
Assignment and directions will be sent prior to attendance
References Daoud, N., Urquia, M. L., O'Campo, P., Heaman, M., Janssen, P. A., Smylie, J., & Thiessen, K. (2012). Prevalence of Abuse and Violence Before, During, and After Pregnancy in a National Sample of Canadian Women. American Journal of Public Health (0), 1-9.
Day Two: 8:00 Questions, pre-test 8:30 Marketing, billing 9:15 Issues of abuse in peripartum 10:15 Break 10:30 Specific diseases, disabilities in peripartum 11:45 LUNCH 12:30 Cultural sensitivity 1:30 Case Studies 2:15 BREAK 2:30 "Ask the Expert" 3:30 Questions, post-test 4:00 Adjourn
Upon completion of this continuing education seminar, participants will be able to: 1. Describe common medical conditions and recommended endocrine function medical tests during the postpartum period. 2. Define the role of physical therapy during labor and delivery. 3. Evaluate, palpate, and treat various nerve dysfunctions in the pelvis related to peripartum issues. 4. List 3 gynecologic surgeries and specific rehabilitation concepts for each. 5. Instruct in safe and effective pregnancy and postpartum exercise techniques using demonstration. 6. Recognize signs of abuse during pregnancy and postpartum and identify the proper means of reporting. 7. Apply connective tissue mobilization techniques to the abdomen and pelvis. 8. Explain common diseases and disabilities that affect a woman and list typical modifications required to support the female patient during pregnancy and postpartum. 9. Identify issues that may arise due to cultural sensitivity and be able to modify approach to therapy as needed to fit a woman’s belief system.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI was born and raised in Duluth, Minnesota. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. She is also a licensed massage practitioner, licensed in Washington since 2003. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and is also certified in Pelvic Rehabilitation and in Pelvic Muscle Dysfunction Biofeedback. Holly served as adjunct faculty at the University of Puget Sound in Tacoma, WA, and at the College of St. Scholastica in Duluth, MN, for whom she continues to teach in the transitional DPT program. Along with H&W faculty member Stacey Futterman she co-authored the "Male Pelvic Floor Function, Dysfunction, and Treatment" course. She is a member of the American Physical Therapy Association and the American Massage Therapy Association. Her physical therapy and massage practice, Flow Rehab, is located in the Fremont neighborhood of Seattle.
Directions from Recommended Lodging to Course Location: (click here if no map appears below)
Attention: We are unable to offer "retro-active" discounts (i.e. applying a discount to a transaction after the transaction takes place), so if you are interested in exploring discount options and you are unsure if your transactions is eligible for a discount, please contact us to inquire.
Multi-Course Discount
This 10% discount is available for a single registrant who wishes to enroll in 3 or more courses, and pay in one transaction. Registrants wishing to enroll in 5 or more courses should contact us for a customized quote. We can also apply this discount if 2 therapists from a single clinic/hospital enroll in 3 or more courses (ie Registrant A enrolls in Course X and Course Y, Registrant B enrolls in Course X, and Registrants A and B both work at Clinic Z). This discount cannot be used in combination with any other discounts. Registration and payment must be received at the same time in one credit card payment, one check or one envelop with multiple checks. This type of registration cannot be completed online, if you are wishing to receive the Multi-Course discount please call or email us directly for assistance.
Course discounts for the Pelvic Floor Series are capped at 10% no matter the group size or number of registrations
Group Discount
This discount is available for a group of three or more registrants, who all work at the same clinic/hospital, enroll in a single course, and pay in a single transaction or mail in multiple checks in a single envelope. This discount cannot be used in combination with any other discounts.
Groups of 3-5 receive a 10% discount off the combined price of their group's registrations.
Course discounts for the PF series are being capped at 10% no matter on group size or number of registrations - but will be staying the same for specialty courses.
Student Discount
This 10% discount is available to current students who have yet to earn a license to practice at the time of course registration. Students are welcome to attend satellite and remote courses with H&W once they have reached their third year and/or completed a hands-on clinical in their second year. You may register while in your 2nd year for a course that is taking place by the time you have become a third-year student. However, students are not allowed to register or attend a self-hosted course.
To get this discount when checking out online, use the code STUDENT2023 for courses scheduled for 2023. (Note, this code is only valid for non-licensed students. The H&W admin team will verify that registrants signed up with this code are, indeed, current students prior to their attendance of the course).
Referral Credit/Discount
Any therapist who has already taken a Herman & Wallace course will earn a $50.00 "referral credit" if:
1. A therapist who has never taken a Herman & Wallace course successfully registers for his or her first course(s); AND 2. In the registration process, the first-time registrant gives the name and clinic/hospital of the therapist who referred them to Herman & Wallace.
A therapist who has earned a $50.00 "referral credit" may use this credit toward any course that is eligible for a "referral discount".
Guest Blogger Credit/Discount
Any therapist who completes a qualifying guest blog post on the Herman & Wallace blog will earn a $50.00 "guest blogger credit". This credit may be applied toward any course.
Holly Tanner is the Director of Education at Herman & Wallace and has curated and instructs the Male Pelvic Floor course. Male Pelvic Floor was first taught in 2008 and has since been expanded to include 22 contact hours. This current content includes 7 pre-recorded lectures and 2 full days of live lectures and labs, allowing more time for hands-on skills in examination and treatment. The schedule covers bladder, prostate, sexual health, and pelvic pain, and further discusses special topics like post-vasectomy syndrome, circumcision, and Peyronie’s disease.
Post-orgasmic illness syndrome (POIS) is a condition that encompasses a cluster of clinical symptoms. The literature most often reports this presentation in men as a response that occurs shortly after ejaculation and that lasts a period of days or even a week or longer. Symptoms may include transient, flu-like symptoms including, but not limited to headache, sore throat, general myalgia, exhaustion, and cognition that is impacted during the reaction. Understandably, people who experience post-orgasm illness often limit sexual encounters, demonstrate avoidance of sexual function, experience interference in relationships with partners, and report lost time from work and other activities. The diagnosis may be primary (occurring from first ejaculation experience) or secondary (acquired later in life.)
Despite the recognition that clinical presentation can be highly variable, diagnostic criteria have been described by Waldinger and colleagues in 2011 (Part 1) and are based on their study of 45 Dutch Caucasian men with POIS.
Preliminary diagnostic criteria for post-orgasmic illness syndrome include 1 or more of the following:
Symptoms occur immediately after or within hours after ejaculation
Symptoms occur almost always, or in more than 90% of ejaculation events
Symptoms last for 2-7 days
Symptoms disappear spontaneously
There are various theories postulating the reason for developing POIS including the autoimmune-allergy hypothesis, cytokine and neuroendocrine disruption, and endogenous m-opioid receptors (orgasm uses large quantities of endogenous opioids). One of the primary reasons that immune reaction to a patient’s own semen has been a strong theory is because sexual activities without ejaculation often do not produce the reaction. Hyposensitization with autologous semen has proven beneficial as a desensitization therapy. (Waldinger et al., 2011, Part 2) Other treatments that may be used include antihistamines, SSRIs, benzodiazepines, and NSAIDs. Comorbidities of POIS reported by Natale and colleagues (2020) include erectile dysfunction, allergies, chronic pelvic pain, autoimmune conditions, and depression and anxiety.
From the standpoint of pelvic rehabilitation, there is much to offer to alleviate symptoms and promote function in patients who have POIS. Genitopelvic pain during or after ejaculation, urinary hesitancy, and difficulty with bowel movements can accompany the syndrome - all complaints that warrant evaluation typical of any patient who has abdominopelvic dysfunction. In the men who have presented to me with this diagnosis, a period of sexual dysfunction including premature ejaculation was described prior to developing POIS. One patient, in particular, described a period of a decade or more of suppressing sexual desires, including masturbation, due to beliefs in his community. When he did masturbate for the first time, he developed post-orgasm illness immediately. I have also observed a tendency to report hypersensitivity to touch, with any palpation to the lower abdomen or groin area causing significant discomfort, and even spontaneous erection or orgasm that was difficult for the patient to manage. In the few cases I have seen, abdominal and pelvic muscle dysfunction was present, and patients responded favorably to manual therapy, education, breathing, and self-management with the use of thermal therapies and self-treatment for soft tissues. It is likely that a combination of medical management, as well as rehabilitation efforts, will provide the best recovery, as anyone who develops fear of an activity usually benefits from learning how to prepare for said activity by addressing concerns prior to, during, and after the activity. Addressing the nervous system response to ejaculation can be part of the rehabilitation process, and a referral to a mental health professional may also prove beneficial in managing the anxiety that often accompanies post-orgasm illness syndrome.
References:
Abdessater, M., Elias, S., Mikhael, E., Alhammadi, A., & Beley, S. (2019). Post orgasmic illness syndrome: what do we know till now?. Basic and Clinical Andrology, 29(1), 1-6.
Le, T. V., Nguyen, H. M. T., & Hellstrom, W. J. (2018). Postorgasmic Illness Syndrome: What do we know so far?. Journal of Rare Diseases Research & Treatment, 3(2).
Nguyen, H. M. T., Bala, A., Gabrielson, A. T., & Hellstrom, W. J. (2018). Post-orgasmic illness syndrome: a review. Sexual Medicine Reviews, 6(1), 11-15.
Waldinger, M. D., Meinardi, M. M., Zwinderman, A. H., & Schweitzer, D. H. (2011). Postorgasmic illness syndrome (POIS) in 45 Dutch Caucasian males: clinical characteristics and evidence for an immunogenic pathogenesis (part 1). The journal of sexual medicine, 8(4), 1164-1170.
Waldinger MD, Meinardi MM, Schweitzer DH. Hyposensitization therapy with autologous semen in two Dutch caucasian males: beneficial effects in Postorgasmic illness syndrome (POIS; part 2). J Sex Med. 2011a;8(4):1171–6
Waldinger, M. D., & Schweitzer, D. H. (2002). Postorgasmic illness syndrome: two cases. Journal of Sex &Marital Therapy, 28(3), 251-255.
Male Pelvic Floor Function, Dysfunction and Treatment - Satellite Lab Course
Description: The course introduces valuable concepts in pelvic health including urinary and prostate function, chronic pelvic pain, and sexual health. For therapists who have taken Pelvic Floor Function, Dysfunction, and Treatment Level 2A, the Men’s Pelvic Health Course expands on the men’s pelvic health topics introduced in Pelvic Floor Level 2A. This continuing education course is also created at an introductory level, covering topics such as internal rectal pelvic muscle examination, so that a therapist who has not taken prior pelvic floor muscle function coursework can attend. It is expected that participants will only register for satellites in which they are within driving distance, and adhere to all state and local COVID guidelines, including wearing a mask at all times during the course.
Urinary dysfunction such as post-prostatectomy incontinence, benign prostatic hypertrophy, urinary retention, and post-micturition dribble are discussed in this class. Because urinary incontinence is a potential consequence following prostate surgery, risk factors, pre-surgical rehabilitation, and post-surgical intervention strategies following prostatectomy are instructed. The medical aspects of prostate cancer testing are also clearly described, including prostate-specific antigen (PSA) testing, Gleason scores, and any recent updates in recommended medical screening.
Although most men diagnosed with prostatitis do not have a true infection, prostatitis remains a common diagnosis within chronic pelvic pain. The Men’s Pelvic Health course explains typical presentations of prostatitis-like pain, evaluation techniques, and evidence-informed intervention techniques. Other pelvic diagnoses are covered, such as Peyronie's Disease, testicular and scrotal pain, penile pain, and pelvic floor muscle-related conditions. Men who experience pelvic muscle dysfunction including pain or weakness are at risk for sexual dysfunction. Participants will be able to describe the relationships between pelvic muscle function and men’s sexual health, including the evidence that demonstrates pelvic muscle rehabilitation's positive impact on erectile function. This continuing education course includes lectures and labs, including external and internal muscle mapping and neuro-myofascial treatment techniques.
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI is a faculty member and the Director of Education at Herman & Wallace. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. Along with H&W faculty member Stacey Futterman, she co-authored the Male Pelvic Floor course.
In the article by Schneider and colleagues (2013) “Refractory chronic pelvic pain syndrome in men: can transcutaneous electrical nerve stimulation help?” the authors conclude that TENS can be effective and safe as a treatment for pelvic pain. What is interesting about the technique they utilize in the intervention is that the electrodes are circumferential, designed to be worn around the penis itself. While this particular treatment may not be of interest for or applicable to all patients with pelvic pain, it may indeed be a valuable tool to add to the list of a comprehensive treatment approach, particularly for the patients who have penile pain or involvement of nerves such as ilioinguinal or the dorsal branch of the pudendal nerve that supplies the penis.
The patients in the report are defined as having “refractory pain” meaning that they have been treated and failed to improve. (Although the definition of “treated” would likely not include a comprehensive pelvic rehabilitation approach.) Patients treated themselves at home for 30 minutes, twice per day at 80 Hz, 150 µs at the sensory threshold level. Outcomes tools included a pain diary using a visual analog scale (VAS) and NIH-CPSI quality of life item at baseline, at 3 months after TENS use, and at last known follow-up appointment. 60 men aged 21-82 years were
Results included successful treatment after 12 weeks in 48% of subjects, and a positive effect was maintained in 21 patients after a mean follow-up of over 43 months. Success meant a greater than 50% reduction in pain VAS and a VAS less than or equal to 3. Pain visual analog scale decreased from 6.6 to 3.9, and QOL improved significantly as well. Fortunately, no adverse events were reported.
While circumferential electrodes are not the only type of electrodes that can be used in pelvic pain TENS application, these electrodes that have a stretchy band to help increased comfort and approximation of the treating surface can allow easy re-use of the electrode and direct placement over the penile tissues. in the image below, one electrode has been placed around the body of the penis and the other is left off simply for viewing the surface of the treatment surface of the electrode. One of 2 leads and electrodes could be used depending on location and extent of pain, and depending on patient preference. Current Medical Technologies carries circumferential electrodes if you are interested in purchasing them.
Although there is no one best treatment pathway for chronic pelvic pain, we can rely on the fact that most patients need multidisciplinary and multimodal support. For conditions that involve overactive nerves or referred pain into the penis, or even for distal treatment for more proximal discomfort, TENS may serve as one “tool in the toolbox” for chronic pelvic, and in particular, chronic penile pain. Pain in the glans, or end of the penis, can be a debilitating and frustrating aspect of pelvic pain (see prior blog post on Pain in the Glans Penis here (link: https://hermanwallace.com/blog/dysfunction-in-glans-penis), and the annoying, distracting sensation of clothing touching the penis can be a source of near-constant irritation. Neuromodulation can be one pathway to assist in moving beyond pain patterns, and it’s a pathway that can be relatively affordable and portable. Because TENS can be applied independently by many patients, TENS can also be a way to improve self-efficacy and provide one strategy for self-care that can be an adjunct to clinical care.
Schneider, M. P., Tellenbach, M., Mordasini, L., Thalmann, G. N., & Kessler, T. M. (2013). Refractory chronic pelvic pain syndrome in men: can transcutaneous electrical nerve stimulation help?BJU Internationa
Holly Tanner, PT, DPT, MA, OCS, WCS, PRPC, LMP, BCB-PMB, CCI is a faculty member and the Director of Education at Herman & Wallace. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. Along with H&W faculty member Stacey Futterman, she co-authored the Male Pelvic Floor course.
In the US, vasectomy is one of the most common procedures performed, and it is often completed in an outpatient setting with a local anesthetic. Fortunately for most folks, it’s well-tolerated and the advice to rest and ice is enough to allow full recovery. Unfortunately, there are those who don’t recover with ease and are left with chronic pain complications. This is a population that is often left out of the clinical rehabilitation setting, and there is not yet robust literature to catch up with the positive clinical results pelvic rehab providers observe when treating post-vasectomy pain.
The Procedure
The goal of a vasectomy is typically contraception. The tube known as either the vas deferens or the ductus deferens is interrupted so that sperm does not travel to its typical destination outside the body via the urethra. This disruption in the tube takes place within the spermatic cord as it passes through the scrotum as this area is easily accessible. There are several techniques that can disrupt the tube where the sperm travels including, but not limited to, clamping, cauterization, or excision. The procedure leaves a small incision in the scrotal tissue.
Post-vasectomy Complications
Complications of a vasectomy may include bleeding and hematoma, infection, sperm granuloma (discussed below), chronic scrotal pain, seminal vesicle abscess (rare), and early or late canalization. (Sihra et al., 2007) Interestingly, some patients report less pain after vasectomy. (Leslie et al., 2007) Theories about the cause of post-vasectomy pain include interstitial fibrosis in the epididymal duct and perineurial fibrosis. (Lee et al., 2012) When we consider the anatomy, within the canal there may also be nerve irritation from the genitofemoral nerve, for example, or other connective tissues. If a patient had pain prior to the procedure in the low back, lower abdomen, or groin, the patient’s system may have been vulnerable to complications due to a sensitized system.
Examination & Rehab Efforts
When a patient presents with pain post-vasectomy, symptoms may worsen with prolonged sitting, with pressure from clothing, or in association with sexual or fitness activities. Because there has been a local insult to the tissues, it is logical to check the site of the procedure for any breakdown, signs of significant inflammation, swelling, and to examine for signs of infection such as fever. (Most patients have returned to their medical provider once pain develops, but if they haven’t, a referral is appropriate.) If the pain can be reproduced locally at the site of the procedure, the pain can often be managed by local treatment. You might find benefit in exam procedures such as a trunk or hip extension for the soft tissue tensioning as well as mechanical loading; palpation to the abdominal wall as well as within the spermatic cord. Treatment can address guarding of the area, general wellness (nutrition, movement, mental health), simple modalities such as heat, and gentle self-mobilization to the painful area.
Granulomas
Granulomas can form following a vasectomy, and while usually asymptomatic, a granuloma may be responsible for post-vasectomy pain. They are described as a “bag-like” structure with disintegrating spermatozoa that form at the cut ends of a vasectomy. (Chatterjee et al., 2001) If the granuloma is painful, very light manual mobilization of the thickened area may be done to alleviate pain (see image below). Mobilization of the spermatic cord itself via the testicle or more proximally may also prove helpful. Local modalities such as ultrasound or heat may improve symptoms as well, but clinically I have found that gentle manual therapy and movement exercises are enough to resolve the pain within a few weeks. Patients can be instructed to complete self-mobilization to the area of the granuloma, and as they often are scared to touch the area, helping alleviate this fear is useful in healing.
Post-vasectomy syndrome is very challenging for patients to manage, as they are often dismissed once the procedure is completed. Patients will share that they have been told “everything looks healed” and that the pain should go away on its own. Most providers are unaware of the role of pelvic rehab clinicians, and many pelvic rehab providers are less knowledgeable about conditions related to the scrotum and spermatic cord. For patients who do not respond to conservative intervention, vasectomy reversals have been found to be significantly helpful in reducing pain, though it’s often undesired due to the goal of contraception that inspired the vasectomy. (Herrel et al., 2015; Polackwith et al., 2015). Ideally, patients will be provided with an early recommendation to pelvic rehab so that further procedures or undoing of the vasectomy is avoided.
If you’d like to learn more about post-vasectomy syndrome and many other conditions that can go unrecognized and under-treated, the next opportunity to take the Male Pelvic Floor course is coming up July 9-10,2021!
Chatterjee, S., Rahman, M. M., Laloraya, M., & Pradeep Kumar, G. (2001). Sperm disposal system in spermatic granuloma: a link with superoxide radicals. International journal of andrology, 24(5), 278-283.
Herrel, L. A., Goodman, M., Goldstein, M., & Hsiao, W. (2015). Outcomes of microsurgical vasovasostomy for vasectomy reversal: a meta-analysis and systematic review. Urology, 85(4), 819-825.
Lee, J. Y., Chang, J. S., Lee, S. H., Ham, W. S., Cho, H. J., Yoo, T. K., ... & Lee, S. W. (2012). Efficacy of vasectomy reversal according to patency for the surgical treatment of postvasectomy pain syndrome. International journal of impotence research, 24(5), 202-205.
Leslie, T.A., R.O. Illing, D.W. Cranston, J. Guillebaud (2007). “The incidence of chronic scrotal pain after vasectomy: a prospective audit.” BJU International 100: 1330-1333.
Polackwich, A. S., Tadros, N. N., Ostrowski, K. A., Kent, J., Conlin, M. J., Hedges, J. C., & Fuchs, E. F. (2015). Vasectomy reversal for postvasectomy pain syndrome: a study and literature review. Urology, 86(2), 269-272.
Fears about treating men’s health conditions are limiting access to care or are creating potential for harm in the field of pelvic health. Many cisgender women (women whose gender identify matches the sex likely assigned at birth) express concerns about working with cisgender men beyond a lack of knowledge about conditions related to prostate issues, urinary leakage, or genital pain. Are these fears warranted, are they fair? Rather than assert that ciswomen should simply move beyond their concerns, the field of pelvic health and the patients with whom we work may be better served by digging in and talking more openly about such fears. Following are some of the concerns or comments I have heard expressed by cisgender women within the context of treating men’s health matters:
(Regarding palpation of the penis:) “Is that legal?”
“I worry about being alone in a room with a man.”
“What if he gets an erection?”
“My husband doesn’t want me to work with other men for pelvic health stuff.”
“I’ve never seen a man’s genitals before and I’m not comfortable with it.”
“My religion teaches that I should not touch a man other than my husband.”
“I don’t know what to say when men make suggestive comments.”
“My supervisor is forcing me to do this work with men when I don’t want to.”
“I only treat them in side lying because then I don’t have to see their stuff.”
Rather than a reader making a judgement about the above comments, we should ask ourselves as a profession if the above topics have been properly addressed in our training or if we are encouraged to work through this area of professional and personal intersecting concerns. We could view the concerns expressed through the lens of providing equal care, in other words, are we discriminating against someone based on their genitals? Or through a lens of safety- is there an actual (as well as perceived) threat from a cisgender woman who is alone in a treatment room with a cisgender man? If that’s potentially true, how are we mitigating this risk? Where does the anatomical line end between personal beliefs such as “I can touch another man’s shoulder, but not perineal area”? Are we practicing ethically if we are denying access to care or providing less than comprehensive care? Is a therapist truly worried about their primary relationship by doing this work because their partner does not approve? And more importantly, can we provide needed guidance or support to address some of the above obstacles?
I commonly have the opportunity to work with men who have seen other self-identified female therapists first. Here is what I often hear:
“I could tell that they weren’t comfortable talking to me about this issue.”
“It didn’t seem like they knew what to do with me.”
“I got switched over to another therapist after asking some questions about using a penile pump.”
“I felt really shamed about my condition because they would change the subject.”
“I called many places and they rejected seeing me because I’m a man.”
“When I asked if they were going to examine where the pain is [genital area] they said it would be a last resort.”
“No one ever examined me, just gave me a biofeedback sensor to put in.”
This information is not shared to shame the caring professionals in our field. What needs to happen, however, for elevating the inclusiveness of care, is a continual dialogue and recognition of the support needed to work with sensitive conditions and the vulnerabilities of both patients and providers. It is potentially harmful to reject patients based on gender, or to provide lesser care based on genitals. To further this conversation, the Institute has partnered with author and educator Leticia Nieto, who holds a degree in psychology and who wrote Beyond Inclusion, Beyond Empowerment: A Developmental Strategy to Liberate Everyone. Join Leticia and me (Holly Tanner) for our first 3-hour discussion that emphasizes talking, feeling, and thinking through some of the above concerns and challenges. The class will focus on discussion more than lecture, and will aim to provide a space within which we can speak openly about how to move forward with the goal of improving comfort when working with men’s health issues and improving access to much needed pelvic health care. Note: this class is welcoming to all people with any gender identification, however, the emphasis will be on the topics discussed in this post.
“However, at present we are all aglow with views on visceral anatomy and medical colleges are wisely establishing chairs in this department which will result in much advancement.” -Fred Byron Robinson, 1891 (Cysts of the Urachus)
The above (fabulous) quote reminds us that many came before us who were equally excited by the study of anatomy. One anatomical structure that I know never appeared in my graduate anatomy courses is the urachus. The urachus is a structure that extends from the urinary bladder to the umbilicus (highlighted blue in the image). When investigating literature about this structure I was impressed to find publications about the urachus dating from the late 19th century.
It wasn’t until several years into my career as a physical therapist that I learned about the urachus, a structure attached to the bladder, and learned how this structure could create some rather dramatic symptoms when in dysfunction. I met a woman who was in her early 30’s and who had 6 months prior undergone a laparoscopic surgery with access just below the umbilicus. She presented to rehabilitation after seeing an urologist for severe pain that occurred towards the end of voiding. The pain was absent at any other time, but was so severe towards the latter half of emptying her bladder that she would double over in pain and “nearly pass out.” Investigation revealed a healthy, well-functioning pelvic floor and abdominal wall, but a reproduction of her severe pain with palpation to the midline between the umbilicus and the pubic bone. After grabbing some anatomy texts, I supposed that the urachus, having potentially been irritated by the laparoscopic approach, might experience a tensioning of the irritated tissue as the bladder contracted to empty. This theory appeared to hold some weight, as applying gentle manual therapy to the tissues, and teaching the patient some self-release techniques allowed her to resolve her symptoms entirely after 1-2 visits.
The urachus is formed in early development from the pre-peritoneal layer, and is described as vestigial tissue. It extends from the anterior dome of the bladder to the umbilicus, varying in length from 3-10 cm, with a diameter of 8-10 mm. There are 3 layers: an inner layer of transitional or cuboid epithelial cells surrounded by a layer of connective tissue. The remains of the urachus form the middle umbilical ligament which is a fibromuscular cord. A layer of smooth muscle that is continuous with the detrusor (smooth muscle of the bladder) makes up the outer layer. This continuity of tissue may help explain some of the clinical connections we see in patient symptoms. In the past year, I have met several patients for whom the urachus is the only tissue that reproduced their symptoms. I examined a male patient who reported urethral burning that occurred with both reset and activity. Unable to produce symptoms in any other location of the thoracolumbar spine, pelvic floor and walls, or abdomen, I palpated this structure to find that it reproduced the urethral burning. Another patient presented with a keloid c-section scar. She also described a sharp pain when the bladder was full. Treatment directed to the scar and along the midline resolved this pain, again with a couple sessions.
If you are interested in learning more about distinct anatomical connections that can help you explain (and treat) issues your patients present with, come and learn with us at the 3-day Male Pelvic Floor Function, Dysfunction, and Treatment course offered four times over the 2019 and 2020 calendars. The role of the urachus in abdominopelvic dysfunction is just one of the many topics we explore. With lectures on sexual health, pelvic pain, prostate and urinary dysfunction, there is a broad range of topics and skills to offer for clinicians who are new to men’s heath and those who have been treating for years.
Begg, R. C. (1930). The Urachus: its Anatomy, Histology and Development. Journal of Anatomy, 64(Pt 2), 170–183. Gray, H. (1918). Anatomy of the Human Body. Philadelphia: Lea & Febiger. Sterling, J. A., & Goldsmith, R. (1953). Lesions of Urachus which Appear in the Adult. Annals of Surgery, 137(1), 120–128.
Managing a medical crisis such as a cancer diagnosis can be overwhelming for an individual. Faced with choices about medical options, dealing with disruptions in work, home and family life often leaves little energy left to consider sexual health and intimacy. Maintaining closeness, however, is often a goal within a partnership and can aid in sustaining a relationship through such a crisis. The research is clear about cancer treatment being disruptive to sexual health, yet intimacy is a larger concept that may be fostered even when sexual activity is impaired or interrupted. Last year, when I was asked to speak to the Pacific NW Prostate Cancer Conference about intimacy, I was pleasantly surprised to find a rich body of literature about maintaining intimacy despite a diagnosis of prostate cancer.
Sexual health and sexuality is a social construct affected by many factors including mood, stress, depression, self-image, physiology, psychology, culture, relational and spiritual factors (Beck et al., 2009; Weiner & Avery-Clark, 2017) Prostate cancer treatment can change relational roles, finances, work life, independence, and other factors including hormone levels.(Beck et al., 2009) Exhaustion (on the part of the patient and the caregiver), role changes, changes in libido and performance anxiety can create further challenges. (Beck et al., 2009; Hawkins et al., 2009; Higano et al., 2012) Recovery of intimacy is possible, and reframing of sexual health may need to take place. Most importantly, these issues need to be talked about, as renegotiation of intimacy may need to take place after a diagnosis or treatment of prostate cancer. (Gilbert et al., 2010)
If the patient brings up sexual health, or we encourage the conversation, there are many research-based suggestions we can provide to encourage recovery of intimacy, several are listed below.
- Manage general health, fitness, nutrition, sleep, anxiety and stress - Redefine sex as being beyond penetration, consider other sexual practices such as massage/touch, cuddling, talking, use of vibrators, medication, aids such as pumps (Usher et al., 2013) - Participate in couples therapy to understand partners’ needs, address loss, be educated about sexual function (Wittman et al., 2014; Wittman et al., 2015) - Participate in “sensate focus” activities (developed by Masters & Johnson in 1970’s as “touch opportunities”) with appropriate guidance (Weiner & Avery-Clark 2017)
Within the context of this information, there is opportunity to refer the patient to a provider who specializes in sexual health and function. While some rehabilitation professionals are taking additional training to be able to provide a level of sexual health education and counseling, most pelvic health providers do not have the breadth and depth of training required to provide counseling techniques related to sexual health- we can, however, get the conversation started, which in the end may be most important.
In the men’s health course, we further discuss sexual anatomy and physiology, prostate issues, and look at the research describing models of intimacy and what worked for couples who did learn to renegotiate intimacy after prostate cancer.
Beck, A. M., Robinson, J. W., & Carlson, L. E. (2009, April). Sexual intimacy in heterosexual couples after prostate cancer treatment: What we know and what we still need to learn. In Urologic oncology: seminars and original investigations (Vol. 27, No. 2, pp. 137-143). Elsevier. Beck, A. M., Robinson, J. W., & Carlson, L. E. (2013). Sexual Values as the Key to Maintaining Satisfying Sex After Prostate Cancer Treatment : The Physical Pleasure–Relational Intimacy Model of Sexual Motivation. Archives of sexual behavior, 42(8), 1637-1647. Gilbert, E., Ussher, J. M., & Perz, J. (2010). Renegotiating sexuality and intimacy in the context of cancer: the experiences of carers. Archives of Sexual Behavior, 39(4), 998-1009. Hawkins, Y., Ussher, J., Gilbert, E., Perz, J., Sandoval, M., & Sundquist, K. (2009). Changes in sexuality and intimacy after the diagnosis and treatment of cancer: the experience of partners in a sexual relationship with a person with cancer. Cancer nursing, 32(4), 271-280. Higano, C. S. (2012). Sexuality and intimacy after definitive treatment and subsequent androgen deprivation therapy for prostate cancer. Journal of Clinical Oncology, 30(30), 3720-3725. Ussher, J. M., Perz, J., Gilbert, E., Wong, W. T., & Hobbs, K. (2013). Renegotiating sex and intimacy after cancer: resisting the coital imperative. Cancer Nursing, 36(6), 454-462. Weiner, L., Avery-Clark, C. (2017). Sensate Focus in Sex Therapy: The Illustrated Manual. Routledge, New York. Wittmann, D., Carolan, M., Given, B., Skolarus, T. A., An, L., Palapattu, G., & Montie, J. E. (2014). Exploring the role of the partner in couples’ sexual recovery after surgery for prostate cancer. Supportive Care in Cancer, 22(9), 2509-2515. Wittmann, D., Carolan, M., Given, B., Skolarus, T. A., Crossley, H., An, L., ... & Montie, J. E. (2015). What couples say about their recovery of sexual intimacy after prostatectomy: toward the development of a conceptual model of couples' sexual recovery after surgery for prostate cancer. The journal of sexual medicine, 12(2), 494-504.
Men who present with chronic pelvic pain frequently have symptoms referred along the penis and into the tip of the penis, or glans. Symptoms may include numbness, tingling, aching, pain, or other sensitivity and discomfort. The tip of the penis, or glans, is a sensory structure, which allows for sexual stimulation and appreciation. This same capacity for valuable sensation can create severe discomfort when signals related to the glans are overactive or irritating. One of the most common complaints with this symptom is a level of annoyance and distraction, with level of bother worsening when a person is less active or not as mentally engaged with tasks. Wearing clothing that touches the tip of the penis (such as underwear, jock straps, jeans, or snug pants) may be limited and may worsen symptoms. When uncovering from where the symptoms originate, the culprit is often the dorsal nerve of the penis, which is sensible given that the glans is innervated by this branch of the pudendal nerve. If we consider this possibility (because certainly there are other potential causes) we find that there are many potential sites of pudendal nerve irritation to consider. First, let’s visualize the anatomy of the nerve.
Following the usually accepted descriptions of the dorsal nerve, we know that it is a terminal branch of the pudendal nerve that primarily is created from the mid-sacral nerves. This can lead us to include the lumbosacral region in our examination and treatment, yet in my clinical experience, there are other sites that more often reproduce pain in the glans. As the dorsal nerve branches off of the pudendal, usually after the location of the sacrotuberous ligament, it passes through and among the urogenital triangle layers of fascia where compression or irritation may generate symptoms.
As the nerve travels towards the pubic bone, it will pass inferior to the pubic bone, a location where suspensory ligaments of the penis can be found as well as pudendal vessels and fascia. This is also a site of potential compression and irritation, and palpation to this region may provide information about tissue health. Below is a cross-section of the proximal penis, allowing us to see where the pudendal nerve and vessels would travel inferior to the pubic bone.
As the dorsal nerve extends along either side of the penis, giving smaller branches along its path towards the glans, the nerve may also be experiencing soft tissue irritation along the length of the penis or even locally at the termination in the glans.
Palpation internally (via rectum) or externally may be a part of the assessment as well as treatment of this condition. Oftentimes, tip of the penis pain can be reproduced with palpation internally and directed towards the anterior levator ani and the connective tissues just inferior to the pubic bone. It may be difficult to know if the muscle is providing referred pain, or if the nerve is being tensioned and reproducing symptoms, however gentle soft tissue work applied to this area is often successful in reducing or resolving symptoms regardless of the tissue involved. In my experience, these symptoms of referred pain at the tip of the penis is often one of the last to resolve, and the use of topical lidocaine may be helpful in managing symptoms while healing takes place. Home program self-care including scar massage if needed, nerve mobilizations, trunk and pelvic mobility and strengthening, and advice for returning to meaningful activities can play a large role in resolution of pain in the glans.
In 2007, after only speaking on the phone and never meeting in person, my new friend and colleague Stacey Futterman and I presented at the APTA National Conference on the topic of male pelvic pain. It was a 3 hour lecture that Stacey had been asked to give, and she invited me to assist her upon recommendation of one of her dear friends who had heard me lecture. I still recall the frequent glances I made to match the person behind the voice I had heard for so many long phone calls.
Upon recommendation of Holly Herman, we took this presentation and developed it into a 2 day continuing education course, creating lectures in male anatomy (we definitely did not learn about the epididymis in my graduate training), post-prostatectomy urinary incontinence, pelvic pain, and a bit about sexual health and dysfunction. Although it truly seems like the worst imaginable question, we asked each other “should we allow men to attend?” As strange as this question now seems, it speaks volumes about the world of pelvic health at that time; mostly female instructors taught mostly female participants about mostly female conditions.
Make no mistake- women’s health topics were and are deserving of much attention in our typically male-centered world of medicine and research. Maternal health in the US is dreadful, and gone are the days when providers should allow urinary incontinence or painful sexual health to be “normal”, yet it is often described as such to women who are brave enough to ask for help. Times have changed for the better for us all.
The Male Pelvic Floor Course was first taught in 2008, and so far, 22 events have taken place in 18 different cities. 73 men have attended the course to date, with increasing numbers represented at each course. Rather than 20-25 attendees, the Institute is seeing more of the men’s health course filling up with 35-40 participants. In my observations, the men who attend the course are often very experienced, have excellent orthopedic and manual therapy skills, and have personalities that fit very well into the sensitive work that is pelvic rehabilitation.
"We are creating male pelvic rehabilitation in real time"
The course was expanded to include 3 days of lectures and labs, and this expansion allowed more time for hands-on skills in examination and treatment. The schedule still covers bladder, prostate, sexual health and pelvic pain, and further discusses special topics like post-vasectomy syndrome, circumcision, and Peyronie’s disease. In my own clinical practice, learning to address penile injuries has allowed me to provide healing for conditions that are yet to appear in our journals and textbooks. As I often say in the course, we are creating male pelvic rehabilitation in real time.
Because the course often has providers in attendance who have not completed prior pelvic health training, instruction in basic techniques are included. For the experienced therapists, there are multiple lab “tracks” that offer intermediate to advanced skills that can be practiced in addition to the basic skills. Adaptations and models are used when needed to allow for draping, palpation, and education when working with partners in lab, and space is created for those therapists who want to learn genital palpation more thoroughly versus those who are deciding where their comfort zone is at the time. One of the more valuable conversations that we have in the course is how to create comfort and ease in when for most us, we were raised in a culture (and medical training) where palpation of the pelvis was not made comfortable. Hearing from the male participants about their bodies, how they are affected by cultural expectations, adds significant value as well.
We need to continue to create more coursework, more clinical training opportunities so that the representation of those treating male patients improves. If you feel ready to take your training to the next level in caring for male pelvic dysfunction, this year there are three opportunities to study. I hope you will join me in Male Pelvic Floor Function, Dysfunction and Treatment.
As someone who has spent nearly two decades marketing myself, my practice, or practices for employers, I have learned a lot of skills by trial and error. One of my favorite strategies to expand my professional network is to “Follow the Patient.” By this I mean to follow the patient to a specialist consult, to a procedure, or to a referral that you helped to coordinate. This must be done with the patient in mind, first and foremost, and then also the provider and their practice environment, so as not to have that practice shut the door on you in the future. Of course, this process can look different if you are in a health network because as an insider, you will likely be more welcome and have all the right credentials in order to simply attend a patient’s provider visit. If you are in a private practice, there are sometimes more hoops and permissions to negotiate. Following are some tips I have learned about this strategy of nurturing referral sources.
Offer the idea to the patient and see if they are open to it. It might sound like this: “If you are interested, I may be able to accompany you to your upcoming appointment. Does that interest you?” It’s very important that the patient is consenting to you being in attendance at their appointment, as the visit is for them. It may be best to not promise that you can clear your schedule, or coordinate the visit, but finding out if the patient is open to the idea is the first step.
2. Check in with the provider’s office. This can be accomplished by you or by the patient. This might sound like this: “I’d like to be sure that your provider would welcome me at your appointment. Would you prefer to contact the provider’s office or shall I?” In my experience, the provider’s office will say “if it’s ok with the patient, it’s fine with us!” Typically, a patient can bring whomever they like to an appointment, so that’s not much of an issue, unless there is close quarters or some other limiting scenario. The good thing about giving a heads up is it allows the provider’s office the opportunity to know that you may be joining your patient. I was able to follow a patient into a hernia repair surgery, and the nurses were so surprised that a physical therapist was in the prep room, they asked me “does the doctor know you are here?” in which case I was able to affirm that I indeed had permission from the surgeon.
3. When you attend the visit, allow the patient to introduce you or politely introduce yourself. Then listen. This is not the time to tell the medical provider all of the wonderful things you have been doing, or all of the things you have to offer their patients. Sometimes when reporting their history, the patient will look questioningly at me to recall details, and unless I am needed to give a brief response, I like to be quiet and stay out of the story until later. This is the time for the patient and the provider to get to know each other, establish rapport, and fewer interruptions are best.
4. Be prepared to summarize your thoughts when given the opportunity to share. Typically I have found that a medical provider will at some point turn and ask me a few questions, or simply state, “Do you have anything to add?” at which point I try to make concise yet thoughtful statements about the patient’s progress, continued challenges, and the reasoning behind the referral if I was the one to coordinate it. The summary might sound like this: “The original severe pain locations have eased, function has improved in this way, and the symptom or issue that is persisting is this. I was interested in knowing if there is potentially something else going on, or if you have a recommendation towards furthering their progress.” At this point, it’s best to not get too far ahead of yourself, or put expectations in front of the patient beyond a brief summary. In other words, don’t request specific imaging or suggest a particular procedure, as this may create an imbalance in the patient’s expectations and the reality of what takes place. If the provider wants more details or thoughts from you, they are likely to ask directly. (You can also send a progress report or summary letter prior to your visit if you have specific thoughts or concerns about what is going on.)
5. Allow the visit to unfold, listen carefully and take mental or written notes. I have often found that I recall details of anatomy, medications, or suggested interventions easily and the patient may ask about the details in a follow-up visit. This type of partnership allows the patient to have “another pair of ears” and can serve as a valuable part of the rehabilitation care planning. For example, perhaps the provider said, “Let’s try this imaging, if nothing of interest shows up, continue rehabilitation for 6 weeks. If no significant progress, I’d like to see you back here within a couple of months from today.” This allows the therapist to note that a provider visit was requested at 6 weeks following the appointment.
Marketing our services, in the long run, and especially in pelvic health, is critical in sharing awareness of the role of pelvic rehabilitation. Marketing is about relationships, and the easiest way to create a relationship is face to face. “Following” a patient along their healing journey, while it may take time out of the clinic for you, is a valuable way of engaging with providers and of being part of a collaborative process. When another provider or therapist requests that I see their patient to offer another view, I find it helpful to welcome the referring therapist to join the patient as well. This can lead to valuable discussions, sharing of information, and ultimately the patient may experience more efficient care that is directed to optimal strategies.
Many therapists transition to treating men with the knowledge and training from female patients. When therapists apply this knowledge, for the most part, it works. When we spend some attention on learning what is a bit different, we might be drawn to the superficial muscles of the perineum. This old anatomy image does a wonderful job of "calling it like it is" or using anatomical terms that describe an action versus naming only the structure. In the image we are looking from below (inferior view) at the perineum and genitals. Just anterior to the anus we can see the anterior muscles within the urogenital triangle, with the base of the shaft of the penis located just anterior to (above in this image) the anus and perineal body. Notice that at the midline, we see muscle names the "accelerator urine". Modern textbooks refer to this muscle as the bulbocavernosus, or bulbospongiosus. Taking the name of accelerator urine, we can understand that this muscle will have an effect on aiding the body in emptying urine. It does this through rhythmic contractions, most often noted towards the end of urination, when the typical spurts of urine follow a more steady stream. This assistance with emptying can take place because the urethra is located within the lower part of the penis, the portion known as the corpus spongiosum. Because the bulbocavernosus muscle covers this part of the penis, and the inferior and lateral parts of the urethra are virtually wrapped within the bulbocavernosus, the muscle can have an effect on emptying the urine in the urethra.
Notice that if you follow the fibers of the accelerator urine muscle towards the top of the image, where the penis continues, you will notice fibers of the muscle wrapping around the sides of the penis. These fibers will continue as a fascial band that travels over the dorsal vessels of the penis. This allows the muscle to also have a significant action during sexual activity, in which blood flow (getting blood into, keeping blood in, and letting blood out of the penis) is paramount.
On either side of the penis we can see what is labeled the erector penis. As these muscles cover the legs, or crura which form the two upper parts of the penis, when the muscles contract, blood is shunted towards the main body of the penis. This of course helps with penile rigidity, as the smooth muscles in the artery walls of the penis allow blood to fill the spongy chambers.
Once we discuss the usual functions of these muscles, we can then imagine the dysfunctions potentially created by less than optimal activity. Consider the difficulty that these muscles will create in contracting or relaxing if they are either too weak, or too tense. These issues can create difficulty emptying well the urethra, often leading to post-void dribble. Blood flow and therefore penile rigidity with erections may be negatively impacted by inability of these muscles to contract or stay contracted, and blood flow leaving the penis may be impaired if the muscles cannot relax. When we work with patients who have genital pain, pelvic floor muscle weakness, dyscoordination, or tension, we can often improve sexual function, bladder emptying, and tasks that might otherwise be affected by pain.
If you are interested in learning more about how to assess and treat these muscles, you have one more opportunity this year to attend the 3-day Male Course instructed by Holly Tanner. Holly has been teaching this course for over 10 years when she co-wrote the first course with colleague and faculty member Stacey Futterman. The course has been updated and turned into a 3-day course to include more manual therapy techniques. Hurry to grab one of the remaining spots in the October 27-29 course in Grand Rapids!

























































 Holly Tanner was born and raised in Duluth, Minnesota, and has lived in Washington state for most of her adult life. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and in Pelvic Rehabilitation. She teaches continuing education courses nationally, teaches in the transitional Doctor of Physical Therapy program for the College of St. Scholastics, and serves as a consultant for practice and program development. She is a member of the American Physical Therapy Association and the American Massage Therapy Association.
Holly Tanner was born and raised in Duluth, Minnesota, and has lived in Washington state for most of her adult life. At Herman & Wallace, Holly is a faculty member and the Director of Education. She owns a private practice that focuses on pelvic rehabilitation and on chronic myofascial pain. She graduated from the College of St. Scholastica in 1995 with a Masters of Arts degree in Physical Therapy and in 2013 she completed a Doctor of Physical Therapy degree. Prior experience includes working for Apple Physical Therapy where she developed and directed the Women's and Men's Health programs for the company’s many clinics. She is Board-certified in Orthopedics, Women's Health, and in Pelvic Rehabilitation. She teaches continuing education courses nationally, teaches in the transitional Doctor of Physical Therapy program for the College of St. Scholastics, and serves as a consultant for practice and program development. She is a member of the American Physical Therapy Association and the American Massage Therapy Association.