
Unfortunately one of the most common things we hear in pelvic rehab is “I hope you can help me, you’re my last hope.” In severe cases, this translates to the patient having little hope of surviving their life with pelvic pain. In severe but not necessarily life-threatening cases, being a patient’s last hope can also mean “please help me have sex in my relationship or my partner is going to leave me.” This situation places a lot of pressure on the patient and also on the therapist. How long did it take this patient to find her way to pelvic rehab? Research tells us that most women have been through multiple physicians, under- or misdiagnosed, and that many have failed attempts at intervention with medications or procedures.
 It’s clear to women that they are being judged when they go to medical appointments complaining of pelvic pain or pain with intercourse. Although it seems really old school to hear that a provider said “It’s all in your head.” or “How much do you like your partner?” or “Well, you’re getting older, sex isn’t that important.” these dismissive phrases are still used. A study by Nguyen et al., 2013 reported that women who reported chronic pain were more likely to perceive being stereotyped by doctors and others. Interestingly, among the group of women who had chronic vulvar pain, the women who sought care for their condition reported feeling more stigmatized. Because the support a woman perceives may influence her willingness to seek out help for chronic vulvar pain, we need to keep educating our peers, the public, and the providers about the real challenges women face, and the power of rehabilitation in overcoming those challenges.
It’s clear to women that they are being judged when they go to medical appointments complaining of pelvic pain or pain with intercourse. Although it seems really old school to hear that a provider said “It’s all in your head.” or “How much do you like your partner?” or “Well, you’re getting older, sex isn’t that important.” these dismissive phrases are still used. A study by Nguyen et al., 2013 reported that women who reported chronic pain were more likely to perceive being stereotyped by doctors and others. Interestingly, among the group of women who had chronic vulvar pain, the women who sought care for their condition reported feeling more stigmatized. Because the support a woman perceives may influence her willingness to seek out help for chronic vulvar pain, we need to keep educating our peers, the public, and the providers about the real challenges women face, and the power of rehabilitation in overcoming those challenges.
Vulvodynia is a common pelvic pain condition, and one that typically is associated with painful intercourse, or dyspareunia. (Arnold et al., 2006) It's estimated that by the age of 40, as many as 8% of women will have or have had a diagnosis of vulvodynia (Harlow et al., 2014), and this is clearly a significant quality of life issue.
Physical therapy has been shown to be successful in treating vulvar pain and pain with intercourse, including as part of a multidisciplinary approach. (Brotto et al., 2015) That's why Herman & Wallace is so eager to help empower more therapists to help patients live a life free of vulvar pain and dyspareunia. You can learn more about our courses and other resources at https://www.hermanwallace.com/continuing-education-courses.
Arnold, L. D., Bachmann, G. A., Kelly, S., Rosen, R., & Rhoads, G. G. (2006). Vulvodynia: characteristics and associations with co-morbidities and quality of life. Obstetrics and gynecology, 107(3), 617.
Brotto, L. A., Yong, P., Smith, K. B., & Sadownik, L. A. (2015). Impact of a multidisciplinary vulvodynia program on sexual functioning and dyspareunia. The journal of sexual medicine, 12(1), 238-247.
Harlow, B. L., Kunitz, C. G., Nguyen, R. H., Rydell, S. A., Turner, R. M., & MacLehose, R. F. (2014). Prevalence of symptoms consistent with a diagnosis of vulvodynia: population-based estimates from 2 geographic regions. American journal of obstetrics and gynecology, 210(1), 40-e1.
Nguyen, R. H., Turner, R. M., Rydell, S. A., MacLehose, R. F., & Harlow, B. L. (2013). Perceived stereotyping and seeking care for chronic vulvar pain. Pain Medicine, 14(10), 1461-1467.

Since the passing of Title IX in 1972, which protects people from sex discrimination in education or activity programs receiving federal funding, the number of females participating in sports has greatly increased. The National Federation of State High School Associations states that in 2011 nearly 3.2 million girls are participating in high school sports.
Unfortunately, a consequence of this increased participation in sports is a higher prevalence in urinary incontinence (UI) and stress urinary incontinence (SUI) in female athletes. Borin et al looked at the ability of nulliparous female athletes to generate intracavity perineal pressure in comparison to nonathletic women. The study demonstrated that higher mean pressures were generated by nonathletic women in comparison to the athletic women group and that lower perineal pressures in the athletic women were also related to number of games per year and time spent on sport specific workouts and strength training workouts.
UI and SUI are underreported in the general population and also in the athletic population. As health care professionals it is important to screen for UI and SUI in our clients. Physical therapy interventions using pelvic floor muscle rehabilitation have shown to decrease the severity of UI and SUI (Rivalta et al, Hulme). Rivalta used internal methods to improve the function of the pelvic floor muscle. Hulme’s success was achieved through activation of the pelvic floor muscles’ extrinsic synergists.
 |
 |
Pilates is often used in physical therapy as a therapeutic tool to improve lumbar stability with studies showing increases in abdominal strength (Sekendiz), trunk extensor endurance (Sekendiz) and to improve posture (Kloubec). Pilates is often also used in pelvic floor muscle rehabilitation and can easily be modified for low level clients. For example the use of resistance can assist supporting the weight of the leg. Practical proof, while lying supine in neutral lumbar spine position, stretch an arm and a leg away from center, notice the difficulty to maintain neutral spine. Now hold a resistance strap, which is also attached to the foot, and notice how maintaining neutral lumbar spine is easier to maintain (pictured above).
Pilates can also be modified for the higher level client or more athletic client. The use of arc barrels, BOSUs or the Hooked on Pilates MINIMAX (pictured belowy) allow the athletic client to achieve an inverted position, unloading the pelvic floor muscles. In the inverted position, pelvic floor muscles may be activated as intrinsic and/or extrinsic synergists of the pelvic floor muscles are also activated. These types of exercises may be more appealing to the athletic client ensuring continuation of the exercise post discharge from physical therapy.
 |
 |
Borin LC, Nunes FR, Guirro EC. Assessment of pelvic floor muscle pressure in female athletes. PMR. 2013; 5(3):189-193.
Hulme, Janet. Beyond Kegels 3rd edition, 2012 Phoenix Publishing Co. Missoula, Montana
Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance and posture. J Strength Cond Res. 2010;24:661-667.
Rivalta M, Sughunolfi MC, Micali S, De Stafani S, Torcasio F, Bianchi G, Urinary incontinence and sport. First and preliminary experience with a combined pelvic floor rehabilitation program in three female athletes. Health Care Women Int. 2010;31(5);330-334.
Sekendiz B, Altun O, Korkusuv F, Akin S, Effects of pilates exercise on trunk strength, endurance and flexibility in sedentary adult females. J Bodyw Mov Ther. 2005;9:52-57.

One of the dilemmas for many clinicians new to pelvic rehab is trying to figure out which equipment to purchase, and how to convince their employer (or themselves) to purchase the equipment. A common question in relation to equipment for pelvic rehabilitation is “what do I really need?” In a perfect world, and based on both existing and emerging research as well as clinical practice recommendations, we would all have access to pressure biofeedback and real-time ultrasound to help us document and train our patients in best strategies. The truth, however, lies in the fact that when those devices are not available, clinical practice can gain meaningful information from our best tools: our eyes and our hands. Certainly when completing research about pelvic floor generated pressures we might choose pressure biofeedback, and when looking for muscle activation patterns, needle EMG is the right choice, but no one should deny patients the opportunity to learn how to increase or decrease muscle activity, focus on movement retraining, and learn strategies to decrease improve quality of life and function because the latest technology is unavailable.
 Recent research published in the Brazilian Journal of Physical Therapy helps affirm the value of vaginal palpation in an article that assessed the relationship between vaginal palpation, vaginal squeeze pressure, electromyography and ultrasound. Eighty women between the ages of 18 and 35 years old, who had never given birth, and who had no known pelvic floor dysfunction were given a thorough evaluation using a multitude of evaluative methods. These methods included vaginal digital palpation (using Modified Oxford scale), vaginal squeeze pressure, electromyographic activity, diameter of the bulbocavernosus muscles as well as bladder neck movement using transperineal ultrasound. The muscles were assessed in a supine, hooklying position. A strong and positive correlation was found between pelvic floor muscle function and pelvic floor muscle contraction pressure. A less strong correlation was found between pelvic muscle function and pressure and electromyography and ultrasound.
Recent research published in the Brazilian Journal of Physical Therapy helps affirm the value of vaginal palpation in an article that assessed the relationship between vaginal palpation, vaginal squeeze pressure, electromyography and ultrasound. Eighty women between the ages of 18 and 35 years old, who had never given birth, and who had no known pelvic floor dysfunction were given a thorough evaluation using a multitude of evaluative methods. These methods included vaginal digital palpation (using Modified Oxford scale), vaginal squeeze pressure, electromyographic activity, diameter of the bulbocavernosus muscles as well as bladder neck movement using transperineal ultrasound. The muscles were assessed in a supine, hooklying position. A strong and positive correlation was found between pelvic floor muscle function and pelvic floor muscle contraction pressure. A less strong correlation was found between pelvic muscle function and pressure and electromyography and ultrasound.
Vaginal pelvic muscle assessment via palpation has been shown to be more accurate when assessed by more experienced therapists, and use of multiple methods may be most valuable in gaining the most accurate data. In addition to validating the usefulness of pelvic muscle palpation as an evaluative tool, the authors point out that transperineal ultrasound may also be the most appropriate tool for pediatric patients or patients who are otherwise not appropriate for internal pelvic muscle assessment.
Pereira, V. S., Hirakawa, H. S., Oliveira, A. B., & Driusso, P. (2014). Relationship among vaginal palpation, vaginal squeeze pressure, electromyographic and ultrasonographic variables of female pelvic floor muscles. Brazilian journal of physical therapy, 18(5), 428-434.

Rarely does a patient with sacroiliac joint dysfunction come to see us with a goal of having surgery. Sometimes surgery winds up being the last resort for relief if our efforts and the patient’s commitment to physical therapy and prescribed exercises fail. Some of the most recent research shows positive results from minimally invasive surgery; however, the bottom line is to make sure the most educated, clinically accurate diagnosis has been made in implicating the SI joint as the source of pain.
Capobianco et al (2015) performed a prospective multi-center trial regarding SI joint fusion using a minimally invasive technique in women with post-partum pain in the pelvic girdle. Eligibility for the study required subjects to have 3 out of 5 positive SI joint stress tests and at least 50% relief with image-guided intra-articular SI joint block with a local anesthetic. Of the 172 subjects in the study, 20 of the 100 females had post-partum pelvic girdle pain, and 52 subjects were male. Significant improvements in pain, quality of life, and function were found for not only the post-partum group but all groups 12 months after surgery. Worth noting is one to three weeks after surgery, the subjects engaged in physical therapy, two times per week for six weeks.
Whang et al (2015) assessed the 6-month outcomes of SI joint fusion using triangular titanium implants versus non-surgical management in a prospective randomized controlled trial. Of the 148 subjects chosen based on similar diagnostic criteria as the study mentioned above, 102 underwent surgery, and 46 had non-surgical management. Non-surgical management involved appropriate pain medication administration, physical therapy, intra-articular SI joint steroid injections, and radiofrequency ablation of sacral nerve roots, all based on individual needs. The surgical group subjects in this study were also asked to have physical therapy two times per week for six weeks anywhere from one to three weeks post-op. The results in a six month follow up showed “clinical success” of >80% in the surgical group and <25% in the non-surgical management group.
The Journal of Neurosurgery: Spine presented an article in July 2015 by Zaidi et al with results of a systematic review of literature regarding the surgical and clinical effectiveness of SI joint fusion. The studies included open as well as minimally invasive surgery, and the causes of surgery included SI joint degeneration and arthritis, SIJ dysfunction, postpartum instability, posttraumatic, idiopathic, pathological fractures, and HLA-B27+/rheumatoid arthritis. A mean rate of satisfaction with open surgery was 54%; whereas, the mean was 84% with minimally invasive surgery. Ultimately, the authors concluded, “serious consideration of the cause of pain” is necessary before embarking on SI joint fusion as the evidence for the surgery’s efficacy is lacking.
So, who is responsible for making the definite diagnosis for SI joint dysfunction? As many patients get minimal time in doctor offices, we have a professional responsibility to competently perform a thorough evaluation for our patients. When the diagnosis is “SI joint dysfunction,” rule out the lumbar spine and hip; and, of course, when “low back pain” or “hip pain” fills the diagnosis line, rule out/in the SI joint. If you are confused about how, it is time to consider taking the Sacroiliac Joint Evaluation and Treatment course!
References:
Capobianco, R., Cher, D., & for the SIFI Study Group. (2015). Safety and effectiveness of minimally invasive sacroiliac joint fusion in women with persistent post-partum posterior pelvic girdle pain: 12-month outcomes from a prospective, multi-center trial. SpringerPlus, 4, 570. http://doi.org/10.1186/s40064-015-1359-y
Zaidi, Hasan A., Montoure, Andrew J., and Dickman, Curits A. (2015). Surgical and clinical efficacy of sacroiliac joint fusion: a systematic review of the literature. Journal of Neurosurgery: Spine. (23)1:59-66. DOI: 10.3171/2014.10.SPINE14516
Whang, P., Cher, D., Polly, D., Frank, C., Lockstadt, H., Glaser, J., … Sembrano, J. (2015). Sacroiliac Joint Fusion Using Triangular Titanium Implants vs. Non-Surgical Management: Six-Month Outcomes from a Prospective Randomized Controlled Trial. International Journal of Spine Surgery, 9, 6. http://doi.org/10.14444/2006

Exercise in pregnancy is a loaded topic. We commonly see images of women doing vigorous exercise in late pregnancy accompanied by judgmental statements about the safety of such activity not only for the woman, but also for the baby. Many myths persist about exercise in pregnancy, and it’s our role as health care specialists to educate women about what is known about exercising. Holly Herman, co-founder of the Herman & Wallace Pelvic Rehabilitation Institute, has been educating providers about this topic for most of her career. Anyone lucky enough to take a course on pregnancy and postpartum issues from Holly Herman knows that her style of teaching is effective and her passion is contagious. From Holly’s use of patient stories to wonderful humor, you can really “get it” when it comes to clinical concepts and strategies. One of Holly’s clinical pearls that really stuck with me after learning about exercise and pregnancy is the research completed by James Clapp in his book “Exercise in Pregnancy”. In short, the book dispels the myth that women shouldn’t exercise in pregnancy and in fact reports on the benefits of exercise to both Mom and baby for labor, delivery, and beyond. In signature style, Holly held this book up in front of the class and to great laughter said, “And this is the book you should buy for your mother-in-law.”
 Another myth that has been perpetuated in relation to pregnancy, labor and delivery is the notion that exercising can make the pelvic floor muscles short, tight, and more narrow, making delivery more difficult. In an article we reported on previously about women being “too tight to give birth” the authors concluded that strong pelvic floor muscles do not lead to challenges with birthing. (Bo et al., 2013) In a more recent article that addressed this issue, Kari Bo and colleagues studied 274 women for levator hiatus (LH) width to see if exercising in late pregnancy did in fact narrow this space. At week 37 of gestation, the exercisers were measured to have a significantly larger LH than the non-exercisers. (Exercisers were defined as women who exercised 30 minutes or more 3 times per week versus the non-exercisers.) The authors conclude that there were not any significant differences in labor outcomes or in delivery outcomes between the groups. (Bo et al., 2015)
Another myth that has been perpetuated in relation to pregnancy, labor and delivery is the notion that exercising can make the pelvic floor muscles short, tight, and more narrow, making delivery more difficult. In an article we reported on previously about women being “too tight to give birth” the authors concluded that strong pelvic floor muscles do not lead to challenges with birthing. (Bo et al., 2013) In a more recent article that addressed this issue, Kari Bo and colleagues studied 274 women for levator hiatus (LH) width to see if exercising in late pregnancy did in fact narrow this space. At week 37 of gestation, the exercisers were measured to have a significantly larger LH than the non-exercisers. (Exercisers were defined as women who exercised 30 minutes or more 3 times per week versus the non-exercisers.) The authors conclude that there were not any significant differences in labor outcomes or in delivery outcomes between the groups. (Bo et al., 2015)
Without a doubt, the patient’s obstetrician gives primary direction to the patient when any high-risk issues are present. Most women however, are basing their exercise choices on experience, on misinformation, myths, or popular opinion. It is our responsibility to engage women in conversations about her health, wellness, and fitness, and to appropriately counsel on exercise during pregnancy and the postpartum period. Most of us lacked proper education about this important population in our primary graduate training, and therefore must seek out information to fill in the gaps. If you are interested in filling in any gaps, join us at one of our peripartum courses around the country. Your next opportunities to take these courses are:
Care of the Postpartum Patient - Seattle, WA
Mar 12, 2016 - Mar 13, 2016
Care of the Pregnant Patient - Somerset, NJ
Apr 30, 2016 - May 1, 2016
Care of the Pregnant Patient - Akron, OH
Sep 10, 2016 - Sep 11, 2016
Bø, K., Hilde, G., Jensen, J. S., Siafarikas, F., & Engh, M. E. (2013). Too tight to give birth? Assessment of pelvic floor muscle function in 277 nulliparous pregnant women. International urogynecology journal, 24(12), 2065-2070.
Bø, K., Hilde, G., Stær-Jensen, J., Siafarikas, F., Tennfjord, M. K., & Engh, M. E. (2015). Does general exercise training before and during pregnancy influence the pelvic floor “opening” and delivery outcome? A 3D/4D ultrasound study following nulliparous pregnant women from mid-pregnancy to childbirth. British journal of sports medicine, 49(3), 196-199.
Clapp, J. F., Cram, C. (2012) Exercising Through Your Pregnancy. Addicts Books

A few years ago, I was convinced my left hip pain was due to osteoarthritis. When my hip locked up after a 14 mile run, my manual therapist husband differentially diagnosed the pain as discogenic. Partly in denial and partly wanting to know the extent of the “damage,” I got an x-ray of my left hip, which was completely normal, and a lumbar MRI, which wasn't pretty. The source of my hip pain was a disc bulge at L3-4 and L4-5 with a Schmorl's node at L5-S1 to boot. Instead of riding the train of thought that we treat what hurts, therapists need to disembark and look further for the source, as suggested in the course, “Finding the Driver in Pelvic Pain.”
 A case report published in the International Journal of Sports Physical Therapy by Livingston, Deprey, and Hensley (2015) documents the discovery of a deeper problem than the referring diagnosis of greater trochanteric pain syndrome. A 29 year old female had to stop running because of lateral hip pain that began 3 months after increasing the intensity and frequency of her running and low impact plyometrics. She had pain in sitting and while running. During the evaluation, she demonstrated a positive Trendelenburg, weak and painless hip abductors, and a positive single leg hop test on concrete. When the pain was not elicited with single leg hop on a foam surface, the patient was referred back to the physician for magnetic resonance imaging. The patient was later diagnosed with an acetabular stress fracture. The therapist’s thorough examination helped prevent possible avascular necrosis or a more traumatic fracture of the pelvis.
A case report published in the International Journal of Sports Physical Therapy by Livingston, Deprey, and Hensley (2015) documents the discovery of a deeper problem than the referring diagnosis of greater trochanteric pain syndrome. A 29 year old female had to stop running because of lateral hip pain that began 3 months after increasing the intensity and frequency of her running and low impact plyometrics. She had pain in sitting and while running. During the evaluation, she demonstrated a positive Trendelenburg, weak and painless hip abductors, and a positive single leg hop test on concrete. When the pain was not elicited with single leg hop on a foam surface, the patient was referred back to the physician for magnetic resonance imaging. The patient was later diagnosed with an acetabular stress fracture. The therapist’s thorough examination helped prevent possible avascular necrosis or a more traumatic fracture of the pelvis.
In a 2013 issue of the same journal, Podschum et al. presents a case report on deciphering the diagnosis in a female runner with deep gluteal pain with pelvic involvement. A 45 year old female marathon runner reported pulling her hamstring and complained of left ischial tuberosity pain with aching into the gluteal and pubic ramus regions that eventually forced her to stop running. She had pain in sitting and could not tolerate speed work. She had a history of low back and pelvic floor pain, with an MRI showing osteitis pubis, a lateral L3-4 bulge, and facet hypertrophy at L4-5. The physical therapist ruled out lumbar disc lesion, radiculopathy, sacroiliac joint dysfunction, and hip labral tear with special tests. Initial treatment focused on the differential diagnoses of hamstring syndrome and ischiogluteal bursitis based on subjective complaints and objective findings. After 4 visits, her deep ache shifted to the inferior pubic ramus in sitting as the ischial tuberosity pain diminished. A trained therapist then conducted a thorough pelvic floor exam. Pelvic floor hypertonic dysfunction was diagnosed and took over the “driver’s seat” as the focus for the rest of the treatment of this patient. Symptoms resolved and the patient returned to running marathons without any of her initial presenting symptoms.
If we let specific pain complaints guide our treatment, we will run out of steam with the lack of progress. Finding the true source of symptoms is critical in physical therapy. Sometimes so much is going on with our patients we have to sort through the weeds before we can access the actual road to recovery. The lumbar spine, hips, and pelvic floor create an intricate map of U-turns and two-way streets, so we need to deepen our understanding of how to navigate the regions. Only then will be able to confidently diagnose the “driver” and let the other areas call “shotgun.”
References:
Livingston, J. I., Deprey, S. M., & Hensley, C. P. (2015). DIFFERENTIAL DIAGNOSTIC PROCESS AND CLINICAL DECISION MAKING IN A YOUNG ADULT FEMALE WITH LATERAL HIP PAIN: A CASE REPORT. International Journal of Sports Physical Therapy, 10(5), 712–722.
Podschun, L., Hanney, W. J., Kolber, M. J., Garcia, A., & Rothschild, C. E. (2013). DIFFERENTIAL DIAGNOSIS OF DEEP GLUTEAL PAIN IN A FEMALE RUNNER WITH PELVIC INVOLVEMENT: A CASE REPORT. International Journal of Sports Physical Therapy, 8(4), 462–471.

Food, at its basic level, provides us with nutrition and sustenance to perform our daily activities. Populations in tune with nature’s cycles of food tend to eat what is available locally based on climate and growth seasons. When societies move beyond simply eating food for energy, but also for flavor, pleasure, and even status, the face of nutrition changes. Whereas some diseases come from a lack of nutrition, many diseases we are faced with in the United States also come from an overabundance of food, with too many calories or too much sugar making up common causes of lack of health. The knowledge within the field of disordered eating is vast, and patients struggling with disordered eating may be fortunate enough to work with a specialist to help recover healthier habits. Even without a diagnosis of disordered eating, many us can identify with unhealthy eating habits, often guided by stress, fatigue, or emotions.
 Prior research has studied how we access willpower under different conditions of cognitive stress. In part of this research, participants were given a number to recall (either 2 digits or 7 digits) and then while walking to another location were offered a snack of either fruit salad or chocolate cake. The authors found that the participants who had to recall a 7 digit number more often chose the chocolate cake, leading the researchers to theorize about the role of higher-level processing and making choices. (Shiv et al., 1999) While we may be aware of a tendency to overeat (or make poorer food choices) during times of stress, fatigue, or emotional distress, changing the habits can be very challenging.
Prior research has studied how we access willpower under different conditions of cognitive stress. In part of this research, participants were given a number to recall (either 2 digits or 7 digits) and then while walking to another location were offered a snack of either fruit salad or chocolate cake. The authors found that the participants who had to recall a 7 digit number more often chose the chocolate cake, leading the researchers to theorize about the role of higher-level processing and making choices. (Shiv et al., 1999) While we may be aware of a tendency to overeat (or make poorer food choices) during times of stress, fatigue, or emotional distress, changing the habits can be very challenging.
“Hunger can be deceptive, and mindfulness can help distinguish emotional from true physical hunger.” -Susan Albers, PsyD
Resources that discuss improving our eating choices in the face of “emotional eating” offers many alternatives, or ways to soothe ourselves without eating. In her books about this topic, clinical psychologist Susan Albers offers advice that may be helpful for our own habit building and for offering basic advice for our patients who struggle with the issue. (While offering advice to patients about healthy eating and habits is within our scope of practice, if a patient has need for a referral to a counselor, psychologist, or nutritionist, we can coordinate such a referral with the patient’s primary care provider.) In her book titled “50 More Ways to Soothe Yourself Without Food: Mindfulness Strategies to Cope with Stress and End Emotional Eating”, Dr. Albers offers many strategies for altering our habits. Some of these ideas include using acupressure points, breathing, rituals, self-massage, yoga, writing, dancing, art, tea, or sex to defer ourselves from poor eating habits. While eating can be enjoyable and pleasurable, when our patients are struggling with over-eating or eating foods that don’t support nutritional or healing goals, having a discussion about these issues may be useful.
If you are interested in learning more about nutrition, consider joining your pelvic rehab colleagues at one of the two Nutrition Perspectives for the Pelvic Rehab Therapist courses this year! Your first chance to attend will be in Kansas City on March 5-6, and later on in Lodi, CA June 25-26.
Albers, S. (2015). 50 More Ways to Soothe Yourself Without Food: Mindfulness Strategies to Cope with Stress and End Emotional Eating. New Harbinger Publications.
Shiv, B., & Fedorikhin, A. (1999). Heart and mind in conflict: The interplay of affect and cognition in consumer decision making. Journal of consumer Research, 26(3), 278-292.
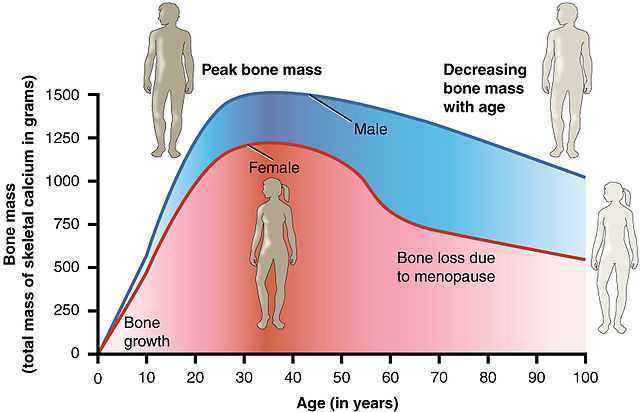
After menopause, more than half of women may have vulvovaginal symptoms that can impact their lifestyle, emotional well being and sexual health. What's more, the symptoms tend to co-exist with issues such as prolapse, urinary and/or bowel problems. But unfortunately many women aren't getting the help they need, despite a growing body of evidence that skilled pelvic rehab interventions are effective in the management of bladder/bowel dysfunctions, POP, sexual health issues and pelvic pain.
 Vaginal dryness, hot flashes, night sweats, disrupted sleep, and weight gain have been listed as the top five symptoms experienced by postmenopausal women in North America and Europe, according to a study by Minkin et al 2015, and they also concluded ‘The impact of postmenopausal symptoms on relationships is greater in women from countries where symptoms are more prevalent.’ Between 17% and 45% of postmenopausal women say they find sex painful, a condition referred to medically as dyspareunia. Vaginal thinning and dryness are the most common cause of dyspareunia in women over age 50. However pain during sex can also result from vulvodynia (chronic pain in the vulva, or external genitals) and a number of other causes not specifically associated with menopause or aging, particularly orthopaedic dysfunction, which the pelvic physical therapist is in an ideal position to screen for.
Vaginal dryness, hot flashes, night sweats, disrupted sleep, and weight gain have been listed as the top five symptoms experienced by postmenopausal women in North America and Europe, according to a study by Minkin et al 2015, and they also concluded ‘The impact of postmenopausal symptoms on relationships is greater in women from countries where symptoms are more prevalent.’ Between 17% and 45% of postmenopausal women say they find sex painful, a condition referred to medically as dyspareunia. Vaginal thinning and dryness are the most common cause of dyspareunia in women over age 50. However pain during sex can also result from vulvodynia (chronic pain in the vulva, or external genitals) and a number of other causes not specifically associated with menopause or aging, particularly orthopaedic dysfunction, which the pelvic physical therapist is in an ideal position to screen for.
According to the North America Menopause Society, ‘…beyond the immediate effects of the pain itself, pain during sex (or simply fear or anticipation of pain during sex) can trigger performance anxiety or future arousal problems in some women. Worry over whether pain will come back can diminish lubrication or cause involuntary—and painful—tightening of the vaginal muscles, called vaginismus. The result can be a vicious circle, again highlighting how intertwined sexual problems can become.’
The research has demonstrated that the optimal strategy for post-menopausal stress incontinence is a combination of local hormonal treatment and pelvic floor muscle training – the strategy of combining the two approaches has been shown to be superior to either approach used individually (Castellani et al 2015, Capobianco et al 2012) and similar conclusions can be drawn for promoting sexual health peri- and post-menopausally.
The pelvic rehab specialist may be called upon to screen for orthopaedic dysfunction in the spine, hips or pelvis, to discuss sexual ergonomics such as positioning or the use of lubricant as well as providing information and education about sexual health before, during and after menopause.
To learn more about sexual health and pelvic floor function/dysfunction at menopause, join me in Atlanta in March for Menopause: A Rehab Approach.
Prevalence of postmenopausal symptoms in North America and Europe, Minkin, Mary Jane MD, NCMP1; Reiter, Suzanne RNC, NP, MM, MSN2; Maamari, Ricardo MD, NCMP3, Menopause:November 2015 - Volume 22 - Issue 11 - p 1231–1238
Low-Dose Intravaginal Estriol and Pelvic Floor Rehabilitation in Post-Menopausal Stress Urinary Incontinence, Castellani D. · Saldutto P. · Galica V. · Pace G. · Biferi D. · Paradiso Galatioto G. · Vicentini C., Urol Int 2015;95:417-421

Occasionally, as pelvic rehab providers, we will encounter the question from our patients, “Do vaginal weights help with urinary incontinence and pelvic floor performance?” The premise behind the use of vaginal cones or balls is that holding them actively in your vagina with your pelvic floor muscles helps to increase the performance (strength and endurance) of the pelvic floor muscles, assisting in reduction of urinary incontinence.
 A recent systematic review (Midwifery, 2015) explores this topic for a specific population of post-partum women with urinary incontinence. The question to be answered was “Does the vaginal use of cones or balls by women in the post-partum period improve performance of the pelvic floor muscles and urinary continence, compared to no treatment, placebo, sham treatment or active controls?”. This review had extensive search criteria. The types of participants in the studies analyzed were post-partum women up to 1 year (when starting interventions) of any parity, that underwent any mode of birth or birth injuries, and had or did not have urinary incontinence. Exclusion criteria were pregnant women, anal incontinence, and major genitourinary/pelvic morbidity. Any frequency, intensity, duration of pelvic exercises with the devices, and any form, size, weight, or brand of vaginal balls or cones were considered. Participants could undergo any type of instruction, either from a health care provider, or self-taught from written materials.
A recent systematic review (Midwifery, 2015) explores this topic for a specific population of post-partum women with urinary incontinence. The question to be answered was “Does the vaginal use of cones or balls by women in the post-partum period improve performance of the pelvic floor muscles and urinary continence, compared to no treatment, placebo, sham treatment or active controls?”. This review had extensive search criteria. The types of participants in the studies analyzed were post-partum women up to 1 year (when starting interventions) of any parity, that underwent any mode of birth or birth injuries, and had or did not have urinary incontinence. Exclusion criteria were pregnant women, anal incontinence, and major genitourinary/pelvic morbidity. Any frequency, intensity, duration of pelvic exercises with the devices, and any form, size, weight, or brand of vaginal balls or cones were considered. Participants could undergo any type of instruction, either from a health care provider, or self-taught from written materials.
Of the searched studies, all were randomized or quasi-randomized controlled trials. The primary outcomes of the searched studies were pelvic floor muscle performance (strength or endurance) and/or urinary incontinence, both assessed with a valid or reliable method. 37 potentially useful articles were reviewed out of 1324 based on the search criteria, but only one article met all of the inclusion criteria and was included in this review with 192 relevant participants (Wilson and Herbison).
In the included study, the group that used vaginal cones (compared to control group) showed a statistically significant lower rate of urinary incontinence. However, when compared to the pelvic exercises group, the continence rates were similar at 12 months post-partum between the cone group and the exercising group. At 24-44 months post-partum, continence rates amongst all groups were similar, but follow-up rates were very low.
As pelvic rehabilitation providers, it is our job to promote pelvic health and assist our post-partum patients with their pelvic impairments, providing them with options to meet their goals. This review does not make a scientific statement of a preferred mode of pelvic exercise, however, it gives us one more option to consider when teaching patients about how to improve pelvic muscle performance to increase urinary continence following child birth. Pelvic exercise enhances pelvic performance, so if your patient would prefer to use vaginal cones or balls to do their pelvic exercise versus completing pelvic exercises without them, do what works best for the patient. One can argue that any pelvic exercise is better than none in improving performance. The use of vaginal cones or balls may be helpful for urinary continence in post-partum women, and provides us with one tool more when promoting pelvic health in our patients.
Oblasser, C., Christie, J., & McCourt, C. (2015). Vaginal cones or balls to improve pelvic floor muscle performance and urinary continence in women post-partum: A quantitative systematic review. Midwifery, 31(11), 1017-1025.
Wilson, P. D., & Herbison, G. P. (1998). A randomized controlled trial of pelvic floor muscle exercises to treat postnatal urinary incontinence. International Urogynecology Journal, 9(5), 257-264.

While working with a 71 year old lady one day, I asked her about her sleep habits, thinking she would describe her neck position, since that it was I was treating. She quickly commented she gets up one to two times every night to use the bathroom. Without any hesitation, she then declared her sister and her friends all do the same thing. No one she knows who is close to her age can sleep through the night without having to pee. Realizing this was more of an issue for my patient than her neck at night, I proceeded to look into the research behind these nighttime escapades of the elderly.
In the Journal of Clinical Sleep Medicine in 2013, Zeitzer et al. performed research regarding insomnia and nocturia in older adults. The introduction explains how 40-70% of older adults experience insomnia, and the greatest cause for sleep disturbance is the need to urinate in the middle of the night (nocturia). In epidemiological studies, between two-thirds and three-quarters older adults report disrupted sleep due to nocturia. The study performed by these authors involved men (average age of 64.3) and women (average age of 62.5) recording their sleep and toileting habits over the course of 2 weeks. The results showed over half the reported awakenings at night were secondary to nocturia. They had worse restfulness and efficiency of sleep associated with the log-reported need to get up to use the bathroom.
 In a 2014 study by Tyagi, et al., the effect of nocturia on the behavioral treatment for insomnia in older adults was explored. The authors noted how nocturia being the primary reason for waking up at night increased proportionately with age with results ranging from 39.9% in people 18-44 years of age to 77.1% in the 65 years old or above population. The 79 participants in this study underwent brief behavioral treatment for their chronic insomnia or only received information. People with and without nocturia both demonstrated significant improvements in quality of sleep after receiving brief behavioral treatment versus the control group; however, the effect size was larger in the participants without nocturia. The authors concluded nocturia needs to be addressed first in order to experience the full benefit of behavior treatment for insomnia.
In a 2014 study by Tyagi, et al., the effect of nocturia on the behavioral treatment for insomnia in older adults was explored. The authors noted how nocturia being the primary reason for waking up at night increased proportionately with age with results ranging from 39.9% in people 18-44 years of age to 77.1% in the 65 years old or above population. The 79 participants in this study underwent brief behavioral treatment for their chronic insomnia or only received information. People with and without nocturia both demonstrated significant improvements in quality of sleep after receiving brief behavioral treatment versus the control group; however, the effect size was larger in the participants without nocturia. The authors concluded nocturia needs to be addressed first in order to experience the full benefit of behavior treatment for insomnia.
On a neurological level, a study from November 2015 by Smith, Kuchel, and Griffiths reported there could be a neural basis for voiding dysfunction in older adults. They found 3 separate neural circuits control voiding, and damage to the pathways feeding these circuits increases with age and can increase urge incontinence. Older adults experiencing neurological deficits may have difficulty discerning what to do when there is urgency and are susceptible to becoming incontinent. The authors recommend treatment of not just the bladder in older people but also therapies to address the structural and functional abnormalities of the neural circuits to provide the greatest results.
So, the next time I saw my patient, I explained to her she is definitely not alone in her nightly rendezvous to the bathroom when it comes to her age group. She has accepted this as “just how things are.” I would like to think there is something more we can do for the elderly population to keep them out of the nocturia “night club.” Taking the Geriatric Pelvic Floor Rehabilitation course by Heather S. Rader, PT, DPT, BCB-PMD, seems like an essential step in the right direction.
Tyagi, S., Resnick, N. M., Perera, S., Monk, T. H., Hall, M. H., & Buysse, D. J. (2014). Behavioral Treatment of Chronic Insomnia in Older Adults: Does Nocturia Matter? Sleep, 37(4), 681–687.
Zeitzer, J. M., Bliwise, D. L., Hernandez, B., Friedman, L., & Yesavage, J. A. (2013). Nocturia Compounds Nocturnal Wakefulness in Older Individuals with Insomnia. Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine, 9(3), 259–262.
Smith, Phillip P., Kuchel, George A., Griffiths, Derek. (2015). Functional Brain Imaging and the Neural Basis for Voiding Dysfunction in Older Adults. Clinics in Geriatric Medicine. 31(4), 549–565.
All Upcoming Continuing Education Courses










Pelvic Function Level 1 - Satellite - Frankfort IL - June 1 - 2 2024 - SOLD OUT
Jun 1 2024 - Jun 2 2024


Pelvic Function Level 1 - Satellite - Columbus OH - June 1 - 2 2024 - SOLD OUT
Jun 1 2024 - Jun 2 2024


Mobilization of the Myofascial Layer Satellite Lab Course - Self-Hosted - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Dry Needling and Pelvic Health - In Person - 3 - Day - Lake Stevens WA - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Kerrville TX - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - East Greenwich RI - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Conyers GA - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Medford OR - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024

Mobilization of the Myofascial Layer Satellite Lab Course - Houston TX - June 7 - 9 2024
Jun 7 2024 - Jun 9 2024


Pelvic Function Level 1 - In-Person - New Haven CT - June 8 - 9 2024 - SOLD OUT
Jun 8 2024 - Jun 9 2024






Pelvic Function Level 2B - Satellite - St. Petersburg FL - June 22 - 23 2024
Jun 22 2024 - Jun 23 2024



Pelvic Function Level 1 - Satellite - Greensboro NC - June 29 - 30 2024 - SOLD OUT
Jun 29 2024 - Jun 30 2024



Pelvic Function Level 1 - Satellite - Torrance CA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024

Pelvic Function Level 1 - Satellite - Philadelphia PA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024

Pelvic Function Level 1 - Satellite - San Diego CA - July 13 - 14 2024 - SOLD OUT
Jul 13 2024 - Jul 14 2024


Modalities and Pelvic Function - In Person - Raleigh NC - July 13 - 14 2024
Jul 13 2024 - Jul 14 2024



Pelvic Function Level 2C - Satellite - King of Prussia PA - July 20 - 21 2024
Jul 20 2024 - Jul 21 2024