

In preparation for this blog, I searched Burnout in the Facebook group Global Health Physio. Here are some snippets. See if you can relate?
“Hello fellow pelvic floor therapists, I would love any guidance or insights about managing the emotional burden of our specialty.”
“I am having internal conflict because I want to give so much more to my patients than time or energy constraints allow.”
“I don't want to survive the workday; I want to thrive and help my patient thrive.”
“I am currently burnt out and have a lot of chronic pain and complex patients on my caseload right now and I just cannot seem to run on time despite not intentionally trying to do this!”
“I'm considering transitioning to at least part time remote in the future to help avoid burnout.”
The struggle is real and relatable.
Then this comment held me in contemplation...
It was my 6th year of being a PT and my first in Pelvic Health when a patient just a bit younger than me sat bawling in my treatment office.
She was bereft. Her fiancé had unceremoniously dumped her and kicked her out of his home. Her mother had estranged her. She had no one and nowhere to go.
I felt my heart beat a little faster as a bit of adrenaline and dopamine hit my bloodstream. A familiar feeling that I interpreted as me about to do a really good thing and help someone (and which I now understand was the chemical “hit” I get with Codependence). I had gotten married 6 months earlier. My husband and I lived in his smallish home, but there was an extra bedroom upstairs. We could help this sweet person!



This specialty of pelvic health has given each of us so many things: purpose, community, and a means to empower and equip so many people to better understand and care for their pelvic health challenges and reach their goals.
But for the rest of the developing world, it’s not like that. Imagine a place where the field of pelvic health simply doesn’t exist. Where women have no choice but to live the rest of their lives with leaking, and community condemnation from birth-induced fistula. Where men suffer in silence with impotence and pelvic pain. Where people with all types of pelvic health conditions must go about their lives hiding and suffering in their private shame.
And then imagine that YOU had the power and influence to change this! To extend your influence, expertise and support all the way across the world to East Africa - to the Amref International University in Nairobi Kenya (AMIU), where even now two cohorts of the FIRST Masters Level Pelvic Health Therapists are busy preparing to revolutionize the understanding and delivery of pelvic rehab in East Africa: Kenya, Uganda, and Ethiopia!
“Is anyone else feeling super burnt out from complex patients right now? I’ve been in pelvic health for 20 years and used to see a lot of easy urinary incontinence patients who all got better fairly quickly. Now all I have is pudendal neuralgia, pelvic pain, and bowel dysfunction. I can’t remember the last SUI patient I had!!”
This week I was tagged in a social media post, that started with the above inquiry…and quickly filled up with thirty-six replies from therapists all over the US, with comments like:
- “The burnout is real.”
- “Mental health issues of today are complicating our patients’ presentations.”
- “Some days I wish for a straightforward TKA.”
- “It’s mentally exhausting.”
- “The simple solutions are rare.”
- “There is so much going on in our world, toxin exposure, stress, work expectations, loneliness, less access to nature and healthy food, less access to being outside…our health is suffering.”
- “The better our skills, the more complex our patients become.”
The last is a favorite. You, dear therapist, INVEST and WORK HARD to EQUIP yourself to serve a population of patients that is ever-increasing in complexity.
Special thanks to faculty member Jennafer Vande Vegte, MSPT, BCB-PMD, PRPC for writing this article. Jen began her career as a physical therapist at Spectrum Health in Grand Rapids, MI she has focused her professional attention on treating women, men, and children with pelvic health disorders since 2002. She has been faculty for Herman & Wallace since 2009 and loves to inspire other rehab professionals treating pelvic floor dysfunction. She is an author of the chapter, “Manual Therapy for the Pelvic Floor” which was published in the book, “Healing in Urology.”
To the physical therapists,


Jennafer Vande Vegte, MSPT, BCB-PMD, PRPC began her career as a physical therapist at Spectrum Health in Grand Rapids, MI. Since 2002 Jen has focused her professional attention on treating women, men, and children with pelvic health disorders. She has been faculty for Herman and Wallace Pelvic Rehabilitation Institute since 2009 and loves to inspire other rehab professionals treating pelvic floor dysfunction. She is an author of the chapter, “Manual Therapy for the Pelvic Floor” which was published in the book, “Healing in Urology.” Jen was a contributing writer for the Pelvic Floor Capstone curriculum and also co-authored the continuing education course, “Boundaries, Self-Care and Meditation” with Nari Clemons.
Do you ever feel like you put more care into treating your patients than do for themselves?
Part 1: Burnout
Let’s get real for a minute.
You are a highly educated professional. If you are reading this blog, I can assume you are invested in your career and your continued education. You are probably pretty skillful, and you help a lot of people.
Faculty members Jenni Gabelsberg DPT, WCS, MSc, MTC and Jennafer Vande Vegte, PT, BCB-PMD, PRPC along with senior Teaching Assistant Quozette Valera PT, DPT will travel to Africa to teach pelvic health in Nairobi City, Kenya through a partnership between Herman & Wallace and The Jackson Foundation. These instructors will be teaching two modules of comprehensive pelvic health training with the goal of creating a self-sustaining, continuous education program taught and offered locally. In addition to training a cohort of physiotherapists in assessing and treating the pelvic floor, these American faculty members will be mentoring local Kenyan therapists to teach these courses in an ongoing manner. We at the Institute are proud and thrilled to be a part of spreading this knowledge and skillset in this currently-underserved region.
The courses offered will comprise H&W's Pelvic Floor Series, with the addition of content relevant to Kenya, including obstetric fistula and female genital mutilation. According to the Worldwide Fistula Fund, there are ~ 2 million women and girls suffering from fistulas. Estimates range from 30 to 100 thousand new cases developing each year; 3-5 cases/1000 pregnancies in low-income countries. A woman may suffer for 1-9 years before seeking treatment. For women who develop fistula in their first pregnancy, 70% end up with no living children.
Have you ever had a dream hidden so deep in your heart you never even spoke it aloud?

I will never forget when my sister, my bestie, told me she wanted to end her life. We were on the phone late one night, tears flowing. Depression was always a companion, but I had never heard her in such a state of despair. We made a plan that she would call the suicide hotline, then call her therapist and her doctor in the morning for urgent care. She made it through the night. Later, I went to her therapist with her so I could better understand and support my sister. She did her due diligence, adjusting medication and staying open and honest in therapy. Suicidal ideations would sometimes flare when there were triggers, but she was able to work through them, and now they are in the past.
Contrast that story with another. Ryan was a sweet woman who developed pudendal neuralgia after a routine hysterectomy. Right away, she told me she had a counselor who she loved who helped her navigate life with DID (Dissociative Identity Disorder) and that I’d probably be interacting with various personalities during our sessions. She helped me understand how to best support her during her care. We worked well together, and although she struggled with both the pain and the unfairness of what happened to her, she was well supported. Then her sweet dog passed away. It was so hard for her. She kept going through pain and heartache and found another pooch to adopt. And then the next visit, she didn’t show. And the next, and the next. And then I found out she was gone. Suicide. This hit me hard. Were there signs that I missed? Was there anything I could have done?
As pelvic rehab providers, we sometimes see people who have intense physical pain often combined with significant emotional wounds. In a study of 713 women seeking support for pelvic pain, 46.8 reported having sexual or physical abuse history, and 31.3 were positive for PTSD (1).
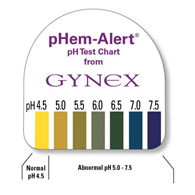
Many years ago a urology doctor shared the skill of testing vaginal pH as part of my pelvic floor exam. I’ve since used it to gather objective data around estrogen status, often finding elevated levels in post-partum, breastfeeding, and peri and post-menopausal women. When correlated with symptoms and visual skin changes this can be a helpful tool to both direct treatment and monitor treatment effectiveness.
To perform pH testing, place a pH strip into the distal vagina. Let it sit there for a few seconds to absorb vaginal moisture. Remove and record results. Any concerning changes in vaginal pH can be documented and reported back to your patient’s medical provider.
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Torrance CA - January 10 - 11 2026 - SOLD OUT
Jan 10 2026 - Jan 11 2026

Oncology of the Pelvic Floor Level 1 - Remote Course - January 10 - 11 2026
Jan 10 2026 - Jan 11 2026

Pelvic Function Level 1 - Satellite - Albany NY - January 10 - 11 2026 - SOLD OUT
Jan 10 2026 - Jan 11 2026


Pelvic Function Level 1 - Satellite - Santa Cruz CA - January 10 - 11 2026
Jan 10 2026 - Jan 11 2026

Pelvic Function Level 1 - Satellite - Huntsville AL - January 10 - 11 2026
Jan 10 2026 - Jan 11 2026



Menopause Transitions and Pelvic Rehab - Remote Course - January 17 - 18 2026
Jan 17 2026 - Jan 18 2026

Pelvic Function Level 1 - Satellite - Bethpage NY - January 24 - 25 2026- SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 2B - Satellite - Port St. Lucie FL - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026


Pelvic Function Level 2B - Satellite - Indianapolis IN - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026


Pelvic Function Level 2B - Satellite - St. Augustine FL - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026




Pelvic Function Level 1 - Satellite - Bradenton FL - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026

Pelvic Function Level 1 - Satellite - New York NY - January 24 - 25 2026 - SOLD OUT
Jan 24 2026 - Jan 25 2026


Pelvic Function Level 1 - Satellite - Los Angeles CA - January 24 - 25 2026
Jan 24 2026 - Jan 25 2026





Pelvic Function Level 1 - In-Person - Columbus OH - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026

Pelvic Function Level 2C - Satellite - Boston MA - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026

Pelvic Function Level 2C - Satellite - Omaha NE - January 31 - February 1 2026
Jan 31 2026 - Feb 1 2026


Pelvic Function Level 1 - Satellite - Fairfax VA - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026

Pelvic Function Level 1 - Satellite - Queens NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026




Pelvic Function Level 1 - Satellite - Greenwich Village NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026



Pelvic Function Level 2B - Satellite - Galloway NJ - February 14 - 15 2026
Feb 14 2026 - Feb 15 2026