Pelvic Rehab Report
The official Herman & Wallace blog. New blogs post every Friday on topics relating to the field of pelvic floor dysfunction.

Elena Teare, the Communications Lead from Open Arms Perinatal Services sat down with The Pelvic Rehab Report to discuss their organization and annual fundraiser Labor of Love.
For our practitioners who are not familiar with Open Arms, can you tell me the organization?
Open Arms is the leading independent, community-based program in Washington State providing wraparound perinatal services to low-income families. We serve nearly 300 families every year and our award-winning program is not hospital-directed or based. Our trusted, community-centered approach always prioritizes the unique cultural, linguistic, and emotional needs of each client free of charge.
We provide services across four program areas: birth doulas, community-based outreach doulas (who provide in-home support up to two years of age), family support services, and lactation support peer counseling. We also train emerging birth workers to serve families in their own communities.
Our communities of focus are Black/African American, Somali, Latinx, and American Indian/Alaska Native communities of King, Snohomish, and Pierce counties. 87% of our clients are of color.

Can you share a success story?
In 2019, Asha was experiencing homelessness when pregnant with her second child. She heard about Open Arms through her shelter and soon was matched with Suad Farole, a Community-Based Outreach Doula. Originally from Somaliher through pregnancy, birth, and her daughter for two years. When Asha became pregnant with her son in late 2020, she knew she wanted Suad to be with her. In Asha’s words, “When I first decided to get a doula, I didn’t expect what I received. Suad was a true gift that not only oversaw the safety of my child as she came into this world, but she truly cared for my well-being and helped me to become the mother that I am now.”
What is the importance of the yearly Labor of Love event?
Labor of Love is our most important fundraising event of the year! It is a chance for us to engage our community and highlight the extraordinary outcomes our families achieve. When community members invest in the work that we do, they provide Open Arms with the flexibility to allocate dollars to any part of the organization that needs extra support. Given the uncertainty in today’s world, it’s important that we have the ability to respond quickly to the changing circumstances of our client families.

What makes you, the staff, volunteers, and the community passionate about this organization?
Our approach is evidence-informed, culturally appropriate, and community-centered and is effective in reducing medical interventions and the costs of perinatal care. By prioritizing the emotional needs of birthing people, our staff and volunteers set the stage for new mothers and parents to be strong and confident advocates for their children and families. By removing the cultural barriers to perinatal care by providing culturally competent care, we facilitate better community linkage to the health care system.
Our doulas and lactation consultants, as well as community of midwives, are committed to improving the health outcomes for birthing people and children of systematically underserved communities. Our families’ outcomes exceed those of Washington state and the country. As of 2021, 95% of our families give birth at full term and healthy birth weight, 85% avoid unplanned cesareans, and 82% are still breast/chestfeeding at six months.[i]
How do persons in need find your organization and what partnerships do you have?
Many of our families are referred from other organizations and service providers, and others find us through word of mouth in the community. Through our Perinatal and Lactation Support Collaborative, we have strong partnerships with the organizations like the Center for Indigenous Midwifery, Generations Midwifery Services, Global Midwifery Services, The Pacific Islander Health Board of Washington, and Rainier Valley Midwives. Additionally, the Program for Early Parenting Support (PEPS) and the Tubman Center for Health and Freedom are additional partnerships we have.

What is the awareness level in the community of Open Arms?
Open Arms clients are referred from other community partners and agencies who trust us to provide the best possible, culturally sensitive care. Over 30% of our referrals are from previous clients who seek our services again or refer friends and family.
How can people who are interested in supporting Open Arms donate or support the organization?
Interested supporters can make a gift to Open Arms online at https://www.openarmsps.org/get-involved/donate/make-gift-today/. To make an even bigger difference in the lives of the families we serve, community members can join our Baby Whisperers Monthly Giving Circle with a sustaining monthly gift. We also value gifts of time and welcome volunteers to assist with some of the behind-the-scenes logistics of the organization. People can stay up to date with our work and opportunities to get involved by heading to our site and subscribing to our newsletter or following our social media channels.

[i] Compared to King county’s rates: 91% of people give birth at full term; 93% are at a healthy birth weight, and 39% are breast/chestfeeding at six months.

Elijah Sharrieff is the content writer for My Community Health Network. MYCHN is a full-service healthcare provider in Houston Texas, that provides accessible health care in multiple Houston Communities. Elijah specializes in blogs that educate patients on relevant topics such as: prenatal care, mental health, the importance of diet and exercise, and dental care. Elijah’s holistic approach to health care blogging stems from his background in education. Elijah taught preschool, middle school, and tutored college and high school students. Teaching allowed Elijah to realize the interconnected nature of health as it relates to the mind and body.
Cervical Health Awareness
Cancer is among the leading causes of death in America. Despite this, cancer is one of those things that you don't think will happen to you. We like to think we are healthy individuals, but cancer is unpredictable and complicated.
Around 300,000 women are diagnosed with cervical precancers in America. MYCHN has created a list of prevention tips to ensure a healthy cervix!
What Causes Cervical Cancer?
Cervical Cancer typically develops when healthy cervix cells grow and multiply continuously. In other words, they don't die like normal cells. Instead, these continually replicating cells form a mass, also known as tumors.
In many cases, HPV can lead to cervical cancer. However, an HPV diagnosis doesn't mean you will be diagnosed with cervical cancer.
What are Cervical Cancer Risk Factors?
Risk factors can increase your cancer risk. There are multiple risk factors for cervical cancer; some of them may surprise you.
- Sexual history: Your sexual history can put you more at risk for cervical cancer.
If you are sexually active at a young age (18 years old and under)
- Diet: If you do not consume a balanced diet, you could be at higher risk for cervical cancer
- Cervical Cancer in the family: If you have family members who have cervical cancer, your chances of developing cervical cancer are higher than if no one in your family has it. In some cases, this is because of rare inherited conditions that make it harder for some women to fight HPV.
- Smoking: It's a difficult habit to quit. However, smoking has been shown to harm the body. Women who smoke are twice as likely to develop cervical cancer.
Tobacco by-products have been found in the cervical mucus of women who smoke. Some studies have shown that the chemicals in cigarettes can damage the DNA of cervix cells. This occurrence can lead to the development of cervical cancer.
How can you Have a Healthy Cervix?
Prevention is going to be vital to lowering your risk of cervical cancer. What are some cervical cancer prevention methods?
- Pap Smear:
A pap smear is a screening that looks for abnormal changes that could lead to cancer. Luckily, cervical cancer doesn't develop overnight, so regular pap smears are useful in cervical cancer prevention.
- Following up with your health care provider:
Following up with your health care provider is crucial to cervical health. Health care providers provide access to pap smears and other preventative measures.
- Get the HPV Vaccine:
The HPV vaccine protects against sub strains of HPV that lead to cervical cancer.
- Limit your sexual partners:
Unfortunately, HPV is easily spread. It is relatively easy to become exposed to HPV. The virus spreads through skin-to-skin contact, so it can be spread without having sex. The American cancer society has stated that HPV can be spread through hand to genital contact.
With the aforementioned in mind, limiting the number of sexual partners could put you at a lower risk of HPV.
- Stop smoking:
Smoking is a tough habit to shake. However, the consequences of smoking are severe for the body's health in the long term. Many cigarettes and tobacco products have harmful cancer-causing chemicals. In addition, smoking weakens your immune system.
A weakened immune system makes it harder for your body to fight viruses like HPV. Just a gentle reminder, HPV can lead to cervical cancer.
Pap Smear Near Me
According to The World Health Organization, cervical cancer is the fourth most common cause of cancer in women. Pap Smears are an excellent cervical cancer prevention method. MYCHN offers pap smears and other women's health services. We have 11 locations in the metropolitan Houston area.
CHN Cares for patients with private insurance, Medicaid, Medicare, and uninsured! Visit https://mychn.org/services/womens-health/ for more.
Bottom Line
Cervical cancer is common cancer for women and, in many cases, can be deadly. Thankfully, there are prevention methods to prevent the disease. For example, regular Pap smears can be used to prevent Cervical cancer.
Eating a balanced diet and not smoking can also be excellent prevention methods.
My Community Health Network. MYCHN is a full-service healthcare provider in Houston Texas, that provides accessible health care in multiple Houston Communities.
References:

Sarah Haran PT, DPT, OCS, CF - L2 earned a BS in exercise science from Gonzaga University and a DPT from the University of Washington. She has been practicing in Seattle for almost 15 years and opened her private practice, Arrow Physical Therapy in 2016. Her specialties include dance medicine, the CrossFit and weightlifting athlete, and conditions of the hip and pelvis such as femoroacetabular impingement and labral tears. In 2017, she began coaching other PTs who wanted to start their own practices and from there, she co-founded Full Draw Consulting with her partner Dr. Kate Blankshain. Together, they offer coaching, consulting, and several 8-week online business courses for Physical Therapy entrepreneurs. Sarah Haran instructs Weightlifting and Functional Fitness Athletes, next scheduled for February 26th, 2022.
As a physical therapist who works with CrossFit® athletes, I want to address a persistent problem we have in our professional community. Many PTs don’t know what to do with CrossFit® athletes.
When CrossFit® first came on the scene, a lot of PTs would encounter athletes who had injuries or dysfunctions related to their sport. Perhaps shoulder pain from kipping pull-ups or low back pain from deadlifts or kettlebell swings, maybe stress incontinence from box jumps.
Whatever it was, it seemed like we were seeing Crossfitter after Crossfitter in our practices. Was it that they were injuring themselves more than other athletes? Was it that their sport was bad and full of terrible ideas and awful coaching? I think what we were seeing was the quick growth of a popular sport (lots of people participating) and a community of people who not only were pushing themselves in the gym but who were interested in getting better and back into the gym quickly (ie. seeking rehab quickly). And then we were seeing rehab professionals who didn’t know how to help and were overwhelmed by the complexity of the sport.
And while there are some folks in healthcare who would like to see CrossFit® lose popularity, the reality is that it is here to stay and you will likely be faced with treating these athletes in some capacity. But what do we do with them? How do we keep our patients healthy when they want to continue to participate in CrossFit®??
The 3 primary duties of the physical therapist:
- Work to understand the sport
- Educate ourselves about where in the body these injuries commonly occur and how they happen
- Design rehab programs:
- ○ which address training volume just as we would in any other sport
- ○ that are functional to these athletes
- ○ that supplement CrossFit® workouts with accessory work to:
-
- ■ drill positions
- ■ strengthen weaknesses
- ■ mobilize tightness
- ■ improve endurance for these positions/movements

The messaging we need to communicate to our CrossFit® patients:
- Form and technique need to come first… then volume, weight, difficulty, and intensity.
- Mobility is not just flexibility; we also need to emphasize stability through a range of motion.
- Scaling and modifying is critical to all athletes at some point in their career. Work with your PT and coach to make appropriate decisions.
- CrossFit® is here to stay. Let’s keep our athletes in this sport for the long haul.
Treating CrossFit® athletes has been a primary passion of mine for many years and it is very exciting to be able to offer a course with Herman & Wallace that introduces the sport to other PTs. You do not have to be a CrossFit® athlete or specialist to want to help these patients and we want all the fabulous PTs out there to be able to impact the CrossFit® community effectively.
Weightlifting and Functional Fitness Athletes will review the history and style of Crossfit exercise and Weightlifting, as well as examine the role that therapists must play for these athletes. Common orthopedic issues presented to the clinic will be examined.
Check out the Herman & Wallace YouTube Channel for the full interview with Dr. Yeni
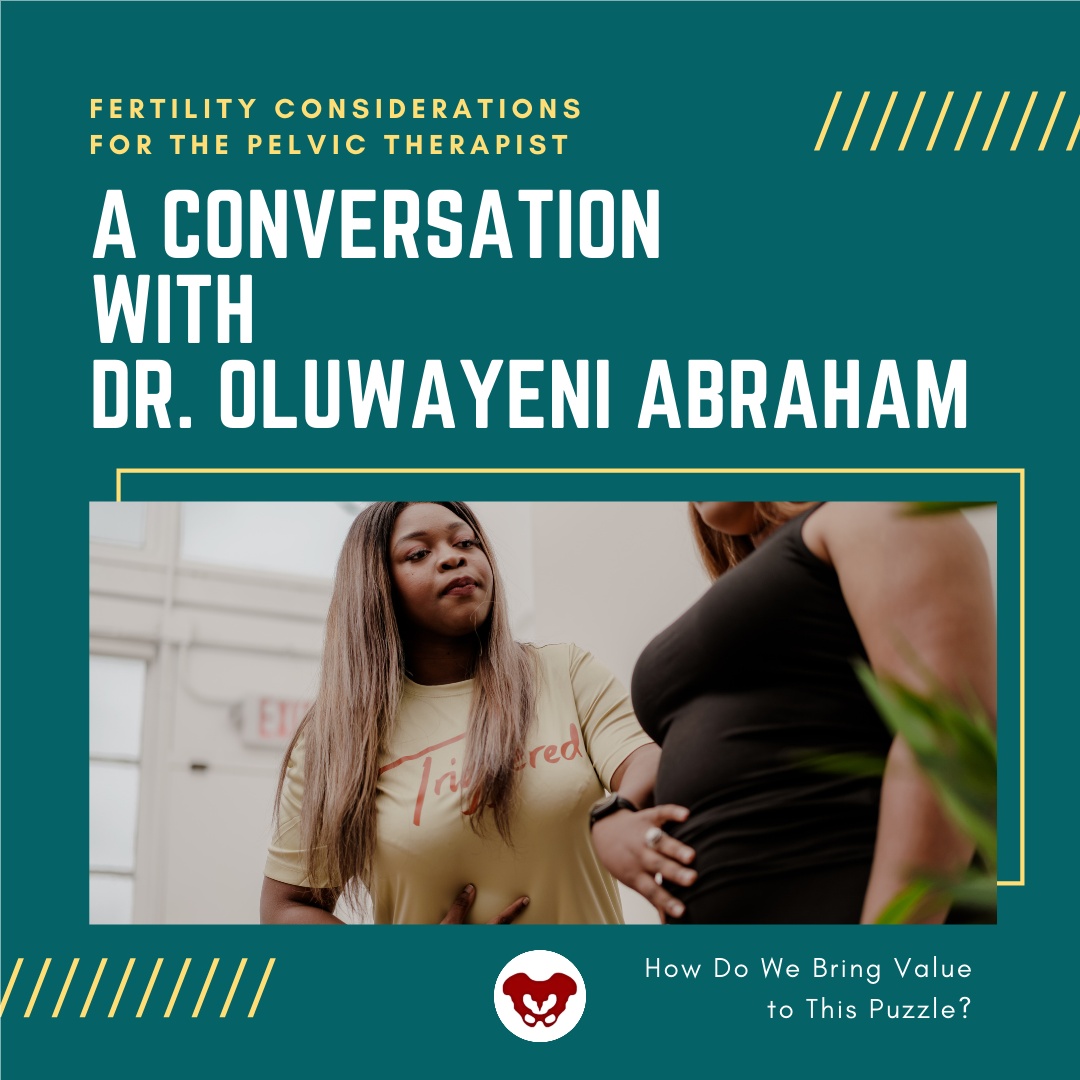
Dr. Oluwayeni Abraham stumbled into the niche field of fertility. She shares, "I had all of these women who would come in with painful periods that would have significant post-surgical problems and would end up having fertility concerns. As I was picking up my visceral mobilization techniques, I started to see that I was able to help women conceive and help women who maybe have experienced reoccurring miscarriages actually carry to term. That's when I said, "I think I'm doing something here that could be something else." That's when I tried to hone in on the specific skills that were influencing and maximizing the results and outcomes.
In Dr. Yeni's course, Fertility Considerations for the Pelvic Therapist, she shares manual therapy techniques and a lot of data on hormones, the endocrine system, and other pieces of the puzzle. The language in the fertility world is based on these building blocks. Specific fertility-related diagnoses are discussed that help you formulate a pathway in treatment. Another important thing Dr. Yeni teaches is how to collaborate and work with these other providers that are going to be on this journey with your patients.
When working with fertility it's important to ask ourselves how do we bring value to this puzzle? How do we bring value after someone has had multiple failed IVF cycles? We can't just say we're going to do a bunch of manual work. We also have to speak the language and understand the body in its entirety and how it's playing a role in being able to maximize fertility outcomes.
When asked what sparks her passion and keeps her so excited about working with this population Dr. Yeni stated, "the outcomes! We're still therapists, and we love to see results."
Fertility Considerations for the Pelvic Therapist - Remote Course
This course requires each registrant to have a live model. Due to the nature of labs, please be sure your model or partner is not pregnant and does not have an IUD for safety. Additionally, those with hydrosalpinx will not be able to participate in uterine mobility techniques but can still attend the course.
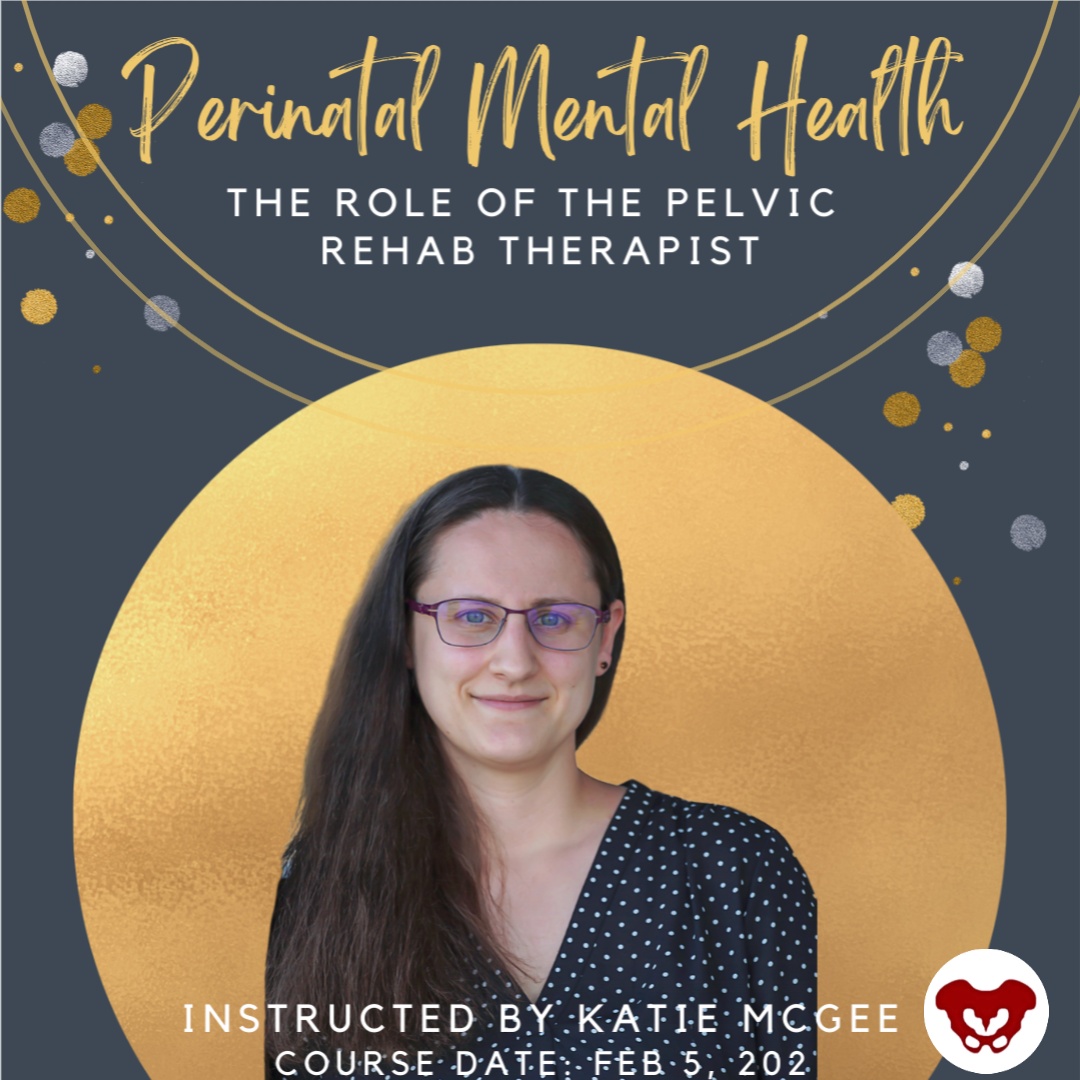
Katie McGee, PT, DPT, (they/them) is a pelvic health physical therapist based in Seattle. Katie received their Doctor of Physical Therapy from the University of Washington in 2014 and their board certification as a Women’s Health Clinic Specialist (WCS) in 2018. Their practice, B3 Physical Therapy, centers on transgender care and perinatal rehabilitation. Join H&W and Katie to learn about perinatal mental health in Perinatal Mental Health: The Role of Pelvic Rehab Therapist - Remote Course scheduled for February 5, 2022.
Due to the COVID-19 pandemic, rates of perinatal mental health conditions—such as anxiety and posttraumatic stress disorder—have risen sharply1. Around 70% of pregnant people are now reporting psychological distress1. With many families under increased stress and financial worry, the odds of developing postpartum depression have jumped from one in seven to one in five(1)!
Fortunately, pelvic rehabilitation therapists can make a difference in the mental health of their perinatal clients. In fact, many pelvic rehab therapists are reducing the risk of perinatal mental health issues without even knowing it! Simply supporting clients in keeping up with physical activity and reducing bodily pain are proven strategies for lowering the risk of perinatal mental health issues (2,3). Pelvic rehab providers can go even further in supporting their perinatal clients’ mental health with some simple actions:
1. Ask – Many birthing people feel shame around negative feelings and thoughts related to pregnancy and postpartum. Asking perinatal clients about their emotional challenges can help break through that shame. A good ice breaker for talking about perinatal mental health is letting your clients know that a mood disorder is the number one complication of pregnancy. Be sure to listen attentively and avoid interruption whenever someone discloses their mental health challenges.
2.Screen – Screening for mental health conditions can guide pelvic rehab therapists to know when it’s time to refer clients to specialized care, such as medication and/or therapy. Pelvic rehab therapists are qualified to use several screening tools in the perinatal period, including the Edinburgh Postnatal Depression Scale, the Patient Health Questionnaire-9, and the Generalized Anxiety Disorder-7. Best of all, these tests are free to use and easy to administer.
3. Gather resources – When a client discloses that they have thoughts of self-harm or are experiencing violence in their home, you want to be prepared with the next steps to help. Collecting resources ahead of time can go a long way in turning what would have been a fumbling offer to help into a confident action plan. Looking to grow your resource list? Check out these three links:
- Perinatal Mental Health Resources: https://www.postpartum.net/
- Intimate Partner Violence Resources: https://www.rainn.org/
- Substance Use Resources: https://www.samhsa.gov/
4. Connect – Racism leads to People of the Global Majority birthing in the United States to experience increased rates of preterm birth and low infant birth weights (4). Both these outcomes have been tied to worse postpartum mental health (5). Research shows that when People of the Global Majority are connected to culturally congruent birth doulas, rates of preterm birth and low infant birth weights fall (6). Other research similarly supports the concept that when people are paired with culturally congruent providers, health outcomes improve (7). Whenever possible, think about how you can offer your clients resources/referrals that match their identity and background to support their mental wellbeing.
5. Learn – Join Katie McGee, PT, DPT (they/them) for the Herman & Wallace course, Perinatal Mental Health: The Role of Pelvic Rehab Therapist - Remote Course scheduled for February 5, 2022. By participating in this remote learning class, you will:
- Develop a basic understanding of perinatal mood and anxiety disorders
- Bolster your listening skills for working with perinatal clients
- Gain additional tips for screening for perinatal mental health issues
- Learn how to help clients create perinatal wellness plans
- Expand your toolbox of coping skills to teach clients
Don’t miss this opportunity to truly change the lives of your perinatal clients!
References
- Yan H, Ding Y, Guo W. Mental Health of Pregnant and Postpartum Women During the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Front Psychol. 2020;11:617001.
- Mathur VA, Nyman T, Nanavaty N, George N, Brooker RJ. Trajectories of pain during pregnancy predict symptoms of postpartum depression. Pain Rep. 2021;6(2):e933.
- Marconcin P, Peralta M, Gouveia ÉR, et al. Effects of Exercise during Pregnancy on Postpartum Depression: A Systematic Review of Meta-Analyses. Biology (Basel). 2021;10(12):1331.
- Andrasfay T, Goldman N. Intergenerational Change in Birthweight: Effects of Foreign-born Status and Race/Ethnicity. Epidemiology. 2020;31(5):649-58.
- Anderson C, Cacola P. Implications of Preterm Birth for Maternal Mental Health and Infant Development. MCN Am J Matern Child Nurs. 2017;42(2):108-14.
- Thomas MP, Ammann G, Brazier E, Noyes P, Maybank A. Doula Services Within a Healthy Start Program: Increasing Access for an Underserved Population. Matern Child Health J. 2017;21(Suppl 1):59-64.
- Towning EJ, Purohit A. Black babies cared for by black doctors less likely to die in the US: revolutionize medical education to tackle the problem in the UK. BMJ. 2020;370:m3783.
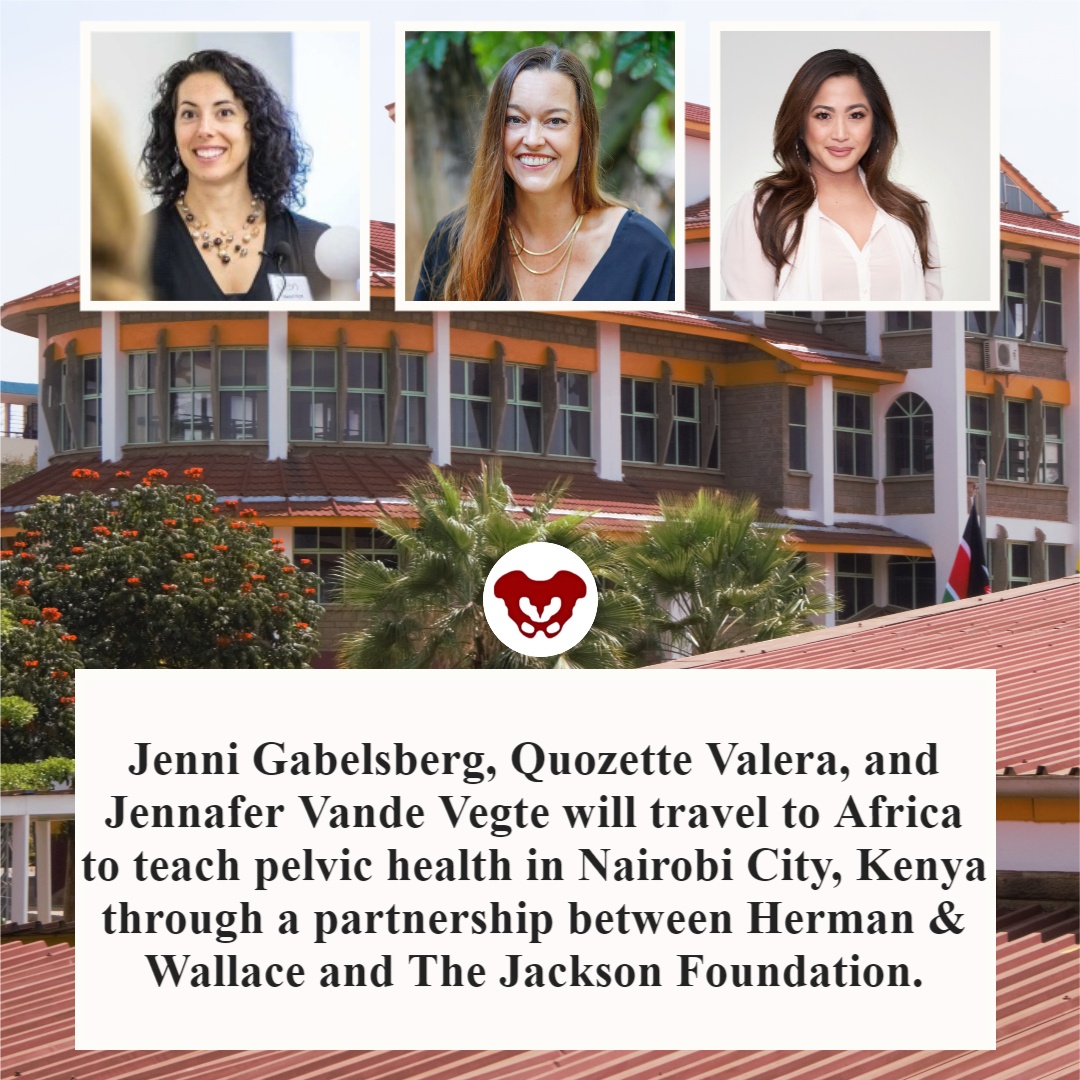
Faculty members Jenni Gabelsberg DPT, WCS, MSc, MTC and Jennafer Vande Vegte, PT, BCB-PMD, PRPC along with senior Teaching Assistant Quozette Valera PT, DPT will travel to Africa to teach pelvic health in Nairobi City, Kenya through a partnership between Herman & Wallace and The Jackson Foundation. These instructors will be teaching two modules of comprehensive pelvic health training with the goal of creating a self-sustaining, continuous education program taught and offered locally. In addition to training a cohort of physiotherapists in assessing and treating the pelvic floor, these American faculty members will be mentoring local Kenyan therapists to teach these courses in an ongoing manner. We at the Institute are proud and thrilled to be a part of spreading this knowledge and skillset in this currently-underserved region.
The courses offered will comprise H&W's Pelvic Floor Series, with the addition of content relevant to Kenya, including obstetric fistula and female genital mutilation. According to the Worldwide Fistula Fund, there are ~ 2 million women and girls suffering from fistulas. Estimates range from 30 to 100 thousand new cases developing each year; 3-5 cases/1000 pregnancies in low-income countries. A woman may suffer for 1-9 years before seeking treatment. For women who develop fistula in their first pregnancy, 70% end up with no living children.
Have you ever had a dream hidden so deep in your heart you never even spoke it aloud?
The dream for me, to someday teach internationally will come to fruition in February 2022. Jenni Gabelsberg DPT, WCS, MSc, MTC; Quozette Valera PT, DPT; and I will travel to Africa to teach pelvic health in Nairobi City, Kenya through a partnership between Herman & Wallace and The Jackson Foundation.
Richard Jackson, a prominent clinician, educator, and businessman himself (The Jackson Clinics, Richard Jackson Seminars, and The Jackson Foundation), had his own dream to build the quality of physical therapy in Africa by educating and empowering clinicians through an evidence-based curriculum developed by Richard and taught by his staff. Richard served two years in the Peace Corps in Kenya in the late 70s. He taught PT at Kenya Medical Training College. In 2010 a former colleague of his moved from the US back to Ethiopia to address and equip PT education and educators in the country. This led to a partnership where Richard helped develop the first DPT program in Africa. “We were in Ethiopia for seven years. We started a residency program that turned into a doctoral program in physical therapy. In December 2017, we graduated 17 DPTs and now we are out. It is sustainable. It’s up to them to carry on and they have the curriculum and the skills,” said Richard in this article.
In 2012 the program Richard stated reproduced and blossomed in Nairobi, Kenya. Let’s talk for a second about what the field of PT is like in Kenya. In a country of almost 54 million people, there are about 2,000 PTs. Thirty-five percent (700) are women, as reported by the Kenya Society of Physiotherapists. The degree is a diploma that takes 3 years to earn, and there are 9 programs available.
There is a women’s health section along with other specialty sections. Medical care has both private and public facilities which can have a wide variation in amenities. After offering specialty training in orthopedics and neurology, Richard recognized the need to expand training to pelvic health. Thus, a partnership between Herman & Wallace, The Pelvic Health and Rehab Center, and The Jackson Foundation was born. In 2019 three cohorts of teachers: Nancy Cullinane PT, MHS, WCS, Kathy Golic PT, and Terri Lannigan PT, DPT, OCS taught module one; Kathy Golic, Casie Danenhauer, and Sherine Aubert fielded a second module; and then educated and equipped the first class of 35 pelvic health graduates. The foundation of the Kenyan Pelvic Health Program thus laid; the future looked bright!
Then…covid brought everything to a screaming halt.
Almost three years later, the program will eagerly resume in Nairobi City.
One can imagine in a country with so few therapists, so few female therapists, and even fewer (think under 50!) pelvic health therapists, the desperate need for pelvic health training and treatment is difficult to fathom. Add to that the strain of a rather patriarchal society where women's health may not be readily accepted or addressed.
In her blog about her experience in Kenya, Sherine Aubert reflects, “To me, this two-week course was way beyond teaching pelvic floor physical therapy - it was truly empowering women to speak up for themselves and each other in the medical community. It provided a voice for anyone suffering from pelvic floor issues to seek help.”
As for Jenni, Quozette, and I, we are beyond humbled and excited to be a part of this experience. Per Richard, "Everyone has come back from these experiences profoundly changed."
If you would like to support this program, we are open to your ideas, expertise, and connections. You can also make a tax-deductible donation to The Jackson Foundation here.
If you have connections to help us bring donations of pelvic health supplies, please contact one of us at This email address is being protected from spambots. You need JavaScript enabled to view it. or This email address is being protected from spambots. You need JavaScript enabled to view it.
For further information:
Read about Richard Jackson.
- https://www.middleburglife.com/world-class-care-at-the-jackson-clinics/
- https://www.orthopt.org/uploads/content_files/files/Jackson.pdf
- https://www.teachandtreat.org/
Read about the 2019 pelvic health training in Kenya:
- https://hermanwallace.com/blog/pelvic-floor-level-1-is-heading-to-kenya
- https://hermanwallace.com/blog/week-one-at-kenya-medical-training-college-in-nairobi-kenya
- https://hermanwallace.com/blog/the-second-course-module-in-nairobi-kenya
Read more about PT in Kenya:
This article was submitted by Aparna Rajagopal and LeeAnn Taptich. Both practitioners are based out of the Henry Ford Macomb Hospital in Michigan where Aparna Rajagopal, PT, MHS is the lead therapist of their pelvic dysfunction program, and Leeann Taptich DPT, SCS, MTC, CSCS leads the Sports Physical Therapy team. Michigan. They work very closely together at the hospital which gives them a very unique perspective of their patients. Aparna and LeeAnn instruct the Breathing and the Diaphragm course. This remote course explores how the diaphragm, breathing, and the abdominals can affect core and postural stability through intra-abdominal pressure changes.
COVID-19 has been a part of our vocabulary for almost 2 years now and has changed the world we live in. COVID-19 is a virus that affects the cardiovascular, digestive, urinary, and respiratory systems. We still do not have adequate evidence to guide our treatment of COVID -19 patients in their sometimes prolonged recovery phase. Research continues to be made available about the short and long-term effects of the virus on our bodies.
An example of a post-COVID-19 patient was a female with complaints of difficulty taking in a deep breath. She also reported that the physical act of breathing felt like a lot of work/effort. She had undergone all sorts of respiratory and cardiac testing and had been cleared from a medical standpoint. Upon talking to the patient, it was discovered that she wasn't complaining of shortness of breath/dyspnea.
Instead, this patient was complaining about having to expend a lot of energy to perform the mechanical action of breathing. She reported that this had started after she had experienced moderate COVID - 19 symptoms for about a month. The patient did extremely well with a plan of treatment aimed at improving mobility in the soft tissues and joints of the thorax while working on establishing a breathing pattern with a focus on improved overall expansion. An incidental benefit of her treatment was a dramatic reduction in her symptoms of urinary urgency which she had developed during her COVID-19 recovery stage.
Recently, a clinical commentary in the Journal of Women’s Health Physical Therapy talked about the possibilities of pelvic floor dysfunction developing on account of COVID-19 (1). Since COVID 19 affects the respiratory system, we can postulate that something involving the respiratory system will possibly have an effect on the pelvic floor due to the unique relationship shared between the pelvic floor and the diaphragm.
Recovering COVID 19 patients may have changes in their musculoskeletal system. These changes may include increased accessory muscle use, decreased chest wall mobility (including the associated joints and muscles), and altered breathing mechanics due to both the disease process and possibly the immobility of bed rest.
The upcoming Breathing and the Diaphragm course helps practitioners understand the connection of dysfunction pertaining to respiration and how it can affect the pelvic floor. In this course, Aparna Rajagopal and LeeAnn Taptich will instruct you to look at the body as a whole while assessing and treating for mobility deficits, motor control deficits in terms of breathing dysfunction presented by these patients.
References:
1. Siracusa C, Gray A. Pelvic floor considerations in COVID-19. Journal of Women’s Health Physical Therapy. 2020; 44(4): 144-151.

Allison Ariail is one of the creators of the Herman & Wallace Oncology of the Pelvic Floor Course Series. Practitioners who took the main Pelvic Floor course still weren’t sure how to handle oncology tissues, what they could do, or how to treat these patients. Thus the oncology series was created to provide additional instruction for treating pelvic cancer patients.
Allison Ariail is a physical therapist who started working in oncology in 2007 when she became certified as a lymphatic therapist. She worked with breast cancer, lymphedema patients, head and neck cancer patients, and the overall oncology team to work with the whole patient to help them get better. When writing these courses, Allison was part of a knowledgeable team that included Amy Sides, Nicole Dugan, Tina Allen, Jennafer Vande Vegte, and Megan Pribyl.
The Oncology Series is comprised of three different courses, with the first course, Oncology of the Pelvic Floor Level 1, designed as an overview of the oncology world. Allison explains that the reason level 1 is an introduction is that “this is because the oncology medical world is so different from what a lot of rehab professionals are used to.”
Oncology of the Pelvic Floor Level 2A addresses colorectal cancers, anal cancers, and cancers that affect male genitalia. New information about how to treat prostate cancers is also discussed. The third course, Oncology of the Pelvic Floor Level 2B, is being launched this year in 2022 and covers gynecological cancers and bladder cancers. The tentative launch will be in November 2022.
There are a lot of labs in all of these courses that are specific to the side effects that these patients have after going through radiation and other surgical treatments. Oncology patients can have a range of problems from radiation fibrosis, range of motion issues, and weakness. While these patients may be seeing a certified lymphatic therapist, that CLT is not going to have time to address these additional issues. Allison Ariail explains, “that is where this knowledge from these courses comes in. Not just as a supplement for that patient, but as a completely different treatment, where that patient really needs to see both therapists. One for lymphedema and one for radiation fibrosis, or weakness, or other side effects, that can affect their quality of life.”
Certified Lymphatic Therapists can skip OPF1 or dive in at OPF2A or OPF2B as long as they have taken the main Pelvic Floor Level 1 course prior.
Oncology of the Pelvic Floor Series 2022 Schedule
Oncology of the Pelvic Floor Level 1
Oncology of the Pelvic Floor Level 2A
Oncology of the Pelvic Floor Level 2B
- TBD – course launch is tentatively scheduled for November 2022
- If you are interested in attending this course, please contact us!

Another circle around the sun.
Another covid pandemic run.
Courses scheduled all year round.
Remote Courses. Live Events, and Satellites abound.
From Oncology and the Pelvic Floor Level 1and Pregnancy Rehabilitation.
To Pain Science for the Chronic Pelvic Pain Population.
Instructors are ready.
With TAs aplenty.
Prove your advanced expertise
And sit for the PRPC.
Our resolution here at Herman & Wallace is to provide even more course content for you! Our plan is to have a total of 22 new courses from 2021-2022 available and over 400 course events/satellites scheduled! In addition, we at H&W want to take the time to let our faculty, teaching assistants, hosts, and students know how much we appreciate you! As the pandemic continues into 2022, know that we see you. We appreciate all that you do and the efforts that you go to.
The best way to make an attainable New Year's Resolution is to use SMART goals. Most of us have seen SMART goals used for work and business decisions. Keep the specific, measurable, and time-specific aspects of goal setting while making sure they are attainable and realistic.
Did you set any New Year's Resolutions yet? If not, then here are 5 suggestions!
- Learn something new. Have fun while challenging yourself to take the next step in your pelvic rehab journey. H&W offers courses that are beginner, intermediate, and advanced levels.
- Build your confidence. Whether it is in gaining confidence in internal exams, or in treating the lumbar nerve H&W has a course for you.
- Meditate & Practice Mindfulness in your personal life and practice. H&W recommends joining Restorative Yoga for Physical Therapists or Boundaries, Self-Care and Meditation.
- Try something that scares you. Push yourself to try things that are out of your comfort zone. Take a new course for a different patient demographic to incorporate into your daily practice such as Bowel Pathology and Function or Transgender Patients: Pelvic Health and Orthopedic Considerations
- Volunteer. Give back to the Pelvic Rehab Community by TA'ing for a satellite course.
Herman & Wallace wishes you a fresh start with renewed energy and confidence throughout the New Year. Happy 2022!

Pelvic rehab therapists and physiatrists both focus on the return to life and function. In a recent interview, Allyson Shrikhande shared, “Physiatrists are extensions of physical therapy. We analyze and treat the muscles, nerves, and joints of the pelvis non-operatively.” Physiatrists bring a holistic viewpoint and are trained to look at the interplay between the different organ systems with each other, as well as the muscles, nerves, and joints.
Dr. Shrikhande is joining H&W to bring in the New Year with her short format course, Working with Physiatry for Pelvic Pain, on January 11th. This 4-hour course delves into diagnosis and non-operative treatment options for Chronic Pelvic Pain (CPPS). Allyson believes in an interdisciplinary team approach to treating patients and spends time discussing the interplay between professions for the betterment of patients.
Physiatrists often work with an interdisciplinary team of rehabilitation experts to coordinate a treatment plan that is based on each patient’s personal needs, abilities, and goals. Members of this interdisciplinary team can include several practitioners:
- Rehabilitation nurses
- Physical therapists
- Occupational therapists
- Respiratory therapists
- Gynecologists
- Dieticians
You can find many clinics and healthcare systems that incorporate a variety of professionals and share a multidisciplinary approach. Multidisciplinary typically means that there are multiple providers but not working together in the same way as interdisciplinary teams. The interdisciplinary approach differs from the multidisciplinary approach by focusing on the common patient and team goals, compared with a discipline-specific focus. It emphasizes regular and effective communication, coordination, and integration of care. Interdisciplinary medical teams are able to work together for functional outcomes (1).
Patients with Chronic Pelvic Pain Syndrome (CPPS) typically experience pain in the abdomen, lower back, and genitals. These patients often experience frequent urination, pain when sitting, and even pain during or after sexual intercourse and impair the function of organs such as the bladder and bowel.
CPPS is a multifaceted disorder. It is a challenge to health care providers because of its unclear etiology and complex natural history. In this case, a pelvic physiatrist may lead an interdisciplinary team including a gynecologist, psychologist, and physical or occupational therapist. In her course, Dr. Shrikhande shares how important it is to understand the pathophysiology of pain. “Experiencing pain for a long period of time changes how the brain receives and processes pain signals. Essentially there is this amplification of pain. This really describes neuroplasticity. The rehab world is founded on neuroplasticity, meaning your peripheral and central nervous system can change in a positive direction or a negative direction.”
Dr. Shrikhande delves into the important role of the physiatrist and pelvic therapist in CPPS treatment in her course Working with Physiatry for Pelvic Pain. Physical and occupational therapists are trained in the clinical features of common musculoskeletal pathology and musculoskeletal examination and develop treatment plans, exercise programs, and physical modalities (including heat, cold, TENS). As a pelvic therapist, an evaluation for CPPS is not just of the pelvic floor. It includes other structures including the abdomen, hip complex, diaphragm, ribcage, low back and looks for weakness, difficulty of coordination, and assessing breathing dysfunction.
As stated by the American Academy of Physical Medicine and Rehabilitation, "Physiatrists, on the other hand, make and manage medical diagnoses and prescribe the therapies that physical and occupational therapists perform. Despite these differences, both therapists and psychiatrists collaborate and communicate to ensure patients are receiving appropriate treatment (2)."
If you have taken Pain Science for the Chronic Pelvic Pain Population, Pudendal Neuralgia and Nerve Entrapment, Yoga for Pelvic Pain, Nutrition Perspectives for the Pelvic Rehab Therapist, Biofeedback for Pelvic Muscle Dysfunction - Satellite Lab Course, or Male Pelvic Floor Function, Dysfunction, and Treatment - Satellite Lab Course you may be interested in attending this course (Working with Physiatry for Pelvic Pain).
Upcoming Working with Physiatry for Pelvic Pain Courses
References:
- Poduri K. R., Vanushkina M. Epidemiology of Aging, Disability, Frailty and Overall Role of Physiatry. Geriatric Rehabilitation. 2018; Pages 1-17. https://doi.org/10.1016/B978-0-323-54454-2.00001-7
- American Academy of Physical Medicine and Rehabilitation. The Medical Student's Guide to PM&R. https://www.aapmr.org/career-support/medical-student-resources/a-medical-students-guide-to-pm-r/what-is-the-difference-between-physical-therapy-and-physiatry
By accepting you will be accessing a service provided by a third-party external to https://hermanwallace.com/
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - Milwaukee WI - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025

Modalities and Pelvic Function - In-Person - Houston TX - July 12 - 13 2025
Jul 12 2025 - Jul 13 2025

Pelvic Function Level 1 - Satellite - Denver CO - July 12 - 13 2025 - SOLD OUT
Jul 12 2025 - Jul 13 2025




Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025









Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Pelvic Function Level 1 - Satellite - Hermosa Beach CA - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
