
Researchers in Norway aimed to determine if an inpatient rehabilitation program (IRP) was superior to an outpatient rehabilitation program (ORP) in helping women return to work following treatment for breast or gynecological cancers. Being unable to work or having to reduce work capacity due to physical and mental challenges is common after cancer treatment. Accompanying changes in quality of life and health status affect women differently and is often based upon diagnoses, treatment interventions completed, education levels and work status, according to the authors. In this article, women attending separate inpatient and outpatient locations with programs designed to reduce drop-out from work by improving physical, psychological, and social health. 51 women were included in the inpatient program, with 50 in the outpatient program. The variables assessed for outcomes included change in work status, fatigue, and health-related quality of life. At time of admission and 6 months post-admission, women ages 18-67 completed the Fatigue Questionnaire (FQ), the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30), and information about work status.
Interventions for both groups included physical exercise, patient education, and group discussions. Educational and group discussions included topics of cancer treatment and side effects, physical activity, nutrition, work rights and return to work issues, partnership and sexuality, psychological reactions to cancer, and coping strategies. The inpatient program involved 3 weeks of stay during the week, and a 1 week follow-up 8-12 weeks later. Educational training comprised approximately 15% of time, group discussions 25% of the time, and physical activity 60% of the time. Exercise activities included Nordic walking, hiking, spinning, stretching, and relaxation. The outpatient rehabilitation occurred 5 hours/day, 1 day/week for 7 weeks. The lectures in the ORP accounted for 25% of the total time, group discussions 25% of the time, and physical activity the remaining 50% of the time. Because of the significant decrease in time spent in rehabilitation, the authors proposed that the subjects in the inpatient program would experience more significant improvements.
Fortunately, both groups improved significantly, without the expected differences in outcomes between groups. In the inpatient program, 73% of the women improved their work status compared to 76% in the outpatient program. All subjects benefited from either program in health-related quality of life and in fatigue, but no significant differences were noted between groups. One reported difference between the intervention groups is that within the inpatient group, an immediate improvement in fatigue was noted. This improvement was attributed to the 1-2 exercise sessions per day in the IRP. The authors conclude that both inpatient and outpatient rehabilitation programs for women following intervention for breast and gynecological cancers can offer substantial benefit. This conclusion is positive in that some patients may not be able to travel to participate in inpatient programs, and the cost of an outpatient program is significantly less than inpatient programs. To learn more about oncological approaches for rehabilitation, the Institute has several courses available. Susannah Haarmann's Breast Oncology course is taking place in February in Arizona. The Oncology and the Pelvic Floor A course (about the female pelvis) is instructed by Michelle Lyons and is offered next in California in May. Check the website for updates to additional oncology course dates. If you are interested in hosting a course, please contact the Institute, and if you would like to be alerted when a particular course is scheduled in your area, let the Institute know and we can keep you informed of schedule updates!


Research published last year in Archives of Gynecology and Obstetrics describes the benefits of "triple therapy" for symptoms of urogenital aging in postmenopausal women. The triple therapy included pelvic floor rehabilitation, intravaginal estradiol, and Lactobacillus acidophili on symptoms of urogenital atrophy, urinary tract infections (UTI's), and stress urinary incontinence (SUI) in postmenopausal women. 136 women with postmenopausal urogenital aging symptoms were divided into two groups of 68 women. Group 1 received intravaginal treatment of combined estriol (30 mcg) and Lactobacillus acidophili (50 mg) and pelvic floor rehabilitation. Group 2 received intravaginal estriol (1 mg) plus pelvic floor rehabilitation. The intravaginal treatment was applied once/day for 2 weeks and then twice/week up to 6 months.
Symptoms of urogenital aging listed by the authors include lower urinary tract issues (urinary frequency and urgency, nocturne, dysuria, recurrent UTI's, and urinary incontinence (UI)), and vaginal or vulval symptoms (vaginal dryness, itching, burning, and dyspareunia.) The connection between the microbiota Lactobacillus acidophili and vaginal health is described in the article involves the proliferation of Lactobacillus acidophili that is stimulated by estrogen. The microbiota then is reproduced in the vaginal epithelium, reduces pH, and prevents colonization of pathogens that can lead to UTI's. The pelvic floor muscle training was completed "…as explained by Castro et al…" in reference to the 2008 study assessing the efficacy of pelvic floor muscle training, vaginal cones, electrical stimulation, and no active treatment. The pelvic floor training in the Castro study included group sessions of pelvic floor muscle contractions as follows: 10 repetitions of 5 seconds contract, 5 seconds relax; 20 repetitions of 2 seconds contract, 2 seconds relax; 20 repetitions of 1 second contract, 1 second relax; 5 repetitions of 10 seconds contract, 10 seconds relax; and 5 simulated cough with strong contraction with 1 minute rest in between.
In the study, the authors assessed outcomes of urogenital symptoms in women aged 55-70 including urine cultures, colposcopic and urethral cytologic findings, urethral pressure profiles, and urethro-cystometry before and 6 months after intervention. Results included that both groups demonstrated significant improvements in symptoms and signs of urogenital atrophy , and 76% of the triple therapy group (Group 1) reported improvement in incontinence versus 41% of Group 2. Subjects in the triple therapy group also were observed to have significant improvements in colposcopic findings, urethral pressure and closure, and in abdominal pressure transmission ratio to the proximal urethra. The study concludes that combination therapy of estriol, Lactobacillus acidophili, and pelvic floor rehabilitation should be considered first-line treatment for postmenopausal symptoms of urogenital aging. To learn more about menopausal evaluation and interventions, check out faculty member Michelle Lyons' new course on Menopause: A Rehabilitation Approach. The next opportunity to take this course is in February in Orlando.
Visceral therapy is used by manual therapists, and research continues to emerge that attempts to explain the underlying mechanisms of the techniques. A study published in the Journal of Bodywork & Movement Therapies in 2012 reports on the effects of visceral therapy on pressure pain thresholds. Osteopathic visceral mobilization was applied to the sigmoid colon in 15 asymptomatic subjects. Pressure pain thresholds were measured at the L1 paraspinal muscles and 1st dorsal interossei before and after intervention. Pressure pain thresholds at the level assessed improved significantly immediately following the visceral mobilization. The effect was not found to be systemic. Hypoalgesia, therefore, may be a mechanism by which visceral mobilization affects patients who are treated with this technique.
Another research study that aimed to assess the effects of visceral manipulation (VM) on low back pain found that the addition of VM to a standard physical therapy treatment approach did not provide short term benefits. However, when the 64 patients were reassessed at 2, 6, and 52 weeks following treatment, the patients in the group with visceral manipulation were found to have less pain at 52 weeks. The patients were randomized into 2 equal groups and were provided physical therapy plus a placebo visceral treatment or a visceral treatment in addition to physical therapy. The authors propose that there may be long-term benefits of including visceral therapy in rehabilitation approaches.
If you would like to learn more about visceral techniques as well as theory and clinical application, check out the updated schedules for Ramona Horton's Visceral Mobilization 1 (VM1): The Urologic System, and Visceral Mobilization 2 (VM2): The Reproductive System. The first opportunity to take VM1 is in January in New Jersey and VM2 is scheduled in September in Ohio.


Women who are diagnosed with and treated for breast cancer commonly suffer from decreased function and fitness, and may be at risk for increased rates of functional decline than women not treated for cancer. This topic is highlighted in a paper published earlier this year in the International Journal of Physical Medicine & Rehabilitation. The authors of this article acknowledge that exercise during and following treatment for breast cancer has significant positive health effects including physical and psychosocial benefits. Cardiorespiratory and resistance training are often recommended to patients as modes of exercise that a breast cancer survivor should participate in, yet the authors raise the question about safety of the recommended exercise programs.
A literature review was completed and in this study 73 studies were included. The studies described exercise programs for patients with breast cancer during treatment and following treatment. The exercise programs within the studies varied widely, with aerobic exercise being prescribed from 10-60 minutes/session, 20-300 minutes/week, at light to vigorous intensity, and with a frequency of 1-7 days/week. The resistance-based exercises, although based on standard exercise principles, also varied dramatically in instructed parameters, according to the authors.
Other key information the authors report from the literature review is that many of the research studies were not representative of the typical patient diagnosed with breast cancer. In fact, as is described in this open-access article, women in the studies were usually younger, had less advanced disease, and in general were more well than the typical patient. For example, listed exclusion criteria in many of the studies included cardiovascular disease, diabetes, COPD, and stroke- some of the most common conditions that a woman with breast cancer also reports.
The take-home point of the article is that because many of the subjects in the exercise studies were not representative of the typical patient with breast cancer, the exercise recommendations may not be appropriate for generalization to most patients during or following treatment for breast cancer. The authors recommend future research considerations that include finding out why women choose to participate in exercise trials or choose to exercise on their own. With so many women simply being given general exercise instructions, the issue of supervised versus unsupervised exercise training, especially for women with more advanced illness should be considered.
If you would like to add more knowledge and skills to your toolbox for treating women diagnosed with breast cancer, you can join faculty member Susannah Haarmann's course Rehabilitation for the Breast Cancer Patient. In 2015 this course is currently scheduled in February in Arizona and in June in Illinois. We hope that you can join us for this specialty course!
Consider the significant numbers of patients who suffer from post traumatic stress disorder, or PTSD. In the pelvic rehabilitation setting, we can think of the patients who may have experienced abuse, a loss of a child, witnessing violence, or other potential precursor. We know from the literature that there is a correlation between traumatic events such as abuse and women who have pelvic pain, within the military population, and among women who experience birth trauma. How then, can we provide patients with self-management tools to address common challenges that accompany PTSD?
Research published online this month in the journal "Mindfulness" states that in patients exposed to trauma, "…those with relatively high levels of mindfulness skills tend to have lower levels of symptoms. The article highlights previous research that has described benefits of mindfulness skills as including decreased anxiety and depression. Mindfulness-based interventions, according to the article, focuses on the development of the skills of awareness (the ability to focus on the here and now, aware of both inner and outer experiences) and acceptance (having a curious, nonjudgmental and open attitude.)
In this study, 101 patients diagnosed by a psychiatrist or psychologist with PTSD completed questionnaires including the Mini-International Neuropsychiatric Interview. The authors found skills in mindfulness correlated negatively with severity of symptoms and with "reactivity" or a tendency to respond with anxiety or depressive thoughts in response to stress. These positive relationships between mindfulness skills and symptoms of PTSD may have a significant impact on many of our patients who suffer from a variety of dysfunctions impacting health.
There is still time to sign up for Carolyn McManus's practical course on mindfulness training. Keep in mind that all therapists (not just pelvic rehab providers) will find this course immediately applicable to their caseload. Join us this November in Seattle for our new offering: Mindfulness-Based Biopsychosocial Approach to Chronic Pain.


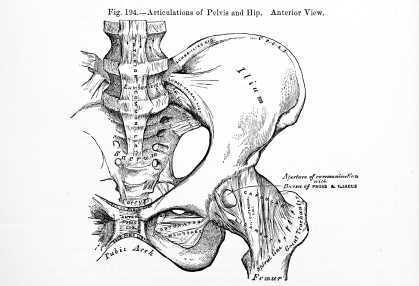
What are the roles of hip labrum innervation in both nociception and proprioception? Canadian researchers tackled this question by studying hip joints that were harvested during total hip replacement or hip resurfacing surgery. Twenty labrums were harvested and the structures in the labrum were divided into four quadrants including antero-superior (AS), postero-superior (PS), antero-inferior (AI), and postero-inferior (PI). The mean age of the subjects was near 60. The authors reported the following:
•Labral innervation is from a branch of the nerve to the quadratus femoris and the obturator nerve.
•All labrum samples had abundant free nerve endings according to the authors. These nerve endings are responsible for nociception transmission.
•Three different types of nerve end organs were noted: Vater-Pacini, Golgi-Mazonian, and Ruffini corpuscles. These nerve end organs operate to provide proprioception through their roles in pressure, deep sensation, and temperature.
•The free nerve endings and nerve end organs were observed more often in the AS and PS zones.
•The nerve endings were noted to be abundant in the superficial zones of the acetabular labrum which were for the most part avascular.
•The antero-superior zone of the labrum has abundant free nerve endings, a fact that correlates with the location of common labral tears and that also fits with the pain produced using a maneuver to test impingement in the hip (flexion, adduction, internal rotation).
•No significant differences in age was noted with respect to the innervation.
The study further states that a labral debridement may ease pain with removal of the free nerve endings, yet the labral repair may best allow for proprioceptive abilities and higher function in the injured hip. The authors also describe the findings that there are abundant myofibroblasts in the labrum that may account for the labrum's ability to heal. To learn more about healing labrums and getting patients moving, check out faculty member Ginger Garner's continuing education course on Extra-Articular Pelvic and Hip Labrum Injury: Differential Diagnosis and Integrative Management. The next opportunity to take the course is in March in Houston.
How long do hot flashes last in a woman's life? One recent study asked this question by following 255 women from premenopause to natural menopause. The authors found that moderate to severe symptoms of hot flashes continued on average 5 years after the date of the woman's last period. Unfortunately, up to 1/3 of the women continued to report hot flashes 10 or more years after menopause. Results also found that risks for hot flashes were higher in women who were African-American or in obese, white women. Higher education level was found to be protective against hot flashes.
The Mayo clinic states that while the exact cause of hot flashes is not known, there are several factors that may influence their occurrence. Changes in reproductive hormones in addition to hypothalamic shifts create a sensitivity to even slight changes in temperature. Women can experience a wide range of menopausal symptoms, with hot flashes ranging from sudden feelings of warmth that occur a couple times per day to profuse sweating that can occur up to one time per hour.
Menopause.org is a helpful resource for our patients, and lifestyle changes are offered such as avoiding stress, breathing techniques, and creating strategies to maintain body temperature within a limited range. Hormonal treatment and non-hormonal options are also described on this site, and while certain hormonal options may be contraindicated for some patients, there are therapies such as sleeping medications that may improve quality of life for a woman who is suffering significant sleep disruption. Decisions to utilize hormonal drug therapy may depend on many factors, such as benefits to risk ratios, if the patient has her uterus, and age of the patient. Many nonprescription options are also available, with conflicting or little evidence to support many of the claims. Regardless of the remedy that a patient may take for her menopausal symptoms, keep in mind that all medications or supplements should be reported to the physician and/or pharmacist so that drug interactions can be screened. Even herbal supplements can have a negative impact on other drugs that a woman is taking, so she should always fully disclose her medications, supplements (including teas!), creams, and other natural remedies.
If you are working with more women in the perimenopausal period, you may have questions about the hormonal changes and effects on rehabilitation. Faculty member Michelle Lyons will offer her new continuing education course called Menopause: A Rehabilitation Approach. At this course she will systemic changes in menopause, bone health, perimenopausal pelvic floor issues, sexual health, weight management, and procedures such as hysterectomy. The next opportunity to take this course is in February in Orlando - what a great time to head to the sunshine!

Avulsion fractures refer to a forcible separation, or tearing away of bone due to a sudden and powerful contraction of muscle. This injury is most common in adolescents, with the as yet developing growth plates being a likely location of avulsion. A systematic review of the literature published in 2011 describes the pathology of pelvic avulsion fractures as "highly prevalent" among adolescent athletes. Additionally, patients who have mature skeletons and who have a history of prior surgical interventions to the bones are also at risk for pelvic avulsion fractures.
Avulsion fractures appear to occur most commonly during the eccentric phase of muscle activity during sporting activities. Pre-existing pain in hip or pelvis may be present, but is not a reliable predictive sign of subsequent fracture. Included in this review article were 48 case reports and case series of which 88% related to physical activity and the remaining 12% related to previous surgical procedures. Within the cases related to physical activity, the mean age of fracture in subjects was 16.8, with 84% being male. Activities in which subjects were involved involved included soccer, gymnastics, and running sports. In the cases related to surgery, mean age of fracture was 56.4, and 100% were female. All of the surgery-related cases presented in the literature were treated with conservative measures. Conservative care described included a period of bed rest for 3 days progressing to walking with crutches until the patient was able to walk without significant pain.
Symptoms reported by patients who have suffered an avulsion fracture of the pelvis may include reporting a popping sensation, local pain, and difficulty walking. Having had a bone harvest from the iliac crest may also predispose a patient to a subsequent avulsion fracture. The authors state that surgery may be considered when there is greater than 2 centimeters of displacement of the avulsion or if the ischial tuberosity is involved.
Rehabilitation therapists should be alert to the age, activity levels, and histories of patients who present with pelvic and hip pain, as an avulsion fracture may be the source of pain. Radiographic imaging will provide further information upon which a plan of care can be made. If you would like to learn more about diagnosing pelvic pain, join your colleagues at one of our courses aimed towards identifying sources of pelvic pain. Peter Philip's continuing education course titled Differential Diagnostics of Chronic Pelvic Pain will next be offered in July of next year in Arlington, VA. Another popular course called Finding the Driver in Pelvic Pain was created by faculty member Elizabeth Hampton and will be offered in April in Milwaukee, WI.


Do women who participate in yoga during pregnancy feel more optimistic, more powerful, and more well? Yes! This is the reply from a study involving 21 women who enrolled in a yoga class for six weeks. While twelve of the women had previously practiced yoga, none were currently practicing. The format of the class involved the following components: checking in (sharing the prior week's experiences), centering (visualization and breathing exercises), warm-up (neck rolls, shoulder exercises, and side stretches), yoga flow (yoga standing positions such as sun salutation), standing postures (balance, wall positions), mat work (seated postures and hip exercises), Savasana (modified to left side lying), and meditation.
Outcomes tools utilized in this study included the Life Orientation Test-Revised for measuring optimism, the Power as Knowing Participation in Change Tool version II for measuring sense of power, the Short-Form 12 Version 2.0, and the Well-being Picture Scale. Participants in the study were also given a journal to document time spent practicing yoga, and how they felt after practicing yoga, both physically and emotionally. The authors conclude that yoga as a self-care practice can be used to promote self-care and well-being in women who are pregnant.
Why are feelings of power, well-being, and optimism valuable for women who are pregnant? The authors discuss the literature which has suggested higher levels of adaptive coping in women with high-risk pregnancies, and the concept that optimism is associated with physical health. Previous studies about using yoga during pregnancy have proposed benefits to the mother both during her pregnancy as well as during labor and delivery. The authors of the study also describe power within the perspective of Rogers' science of unitary human beings, with sharing of interesting philosophical concepts such as resonancy, integrality, and diversity of the human-environmental field.
Because yoga is a popular activity with pregnant women, the study adds to the growing body of research about yoga in the peripartum period. If you are interested in learning how to apply yoga concepts for patients who are pregnant, come to Ginger Garner's continuing education course Yoga As Medicine for Pregnancy and the next opportunity to take this course is next month in New York!
Earlier this year, the Food and Drug Administration issued a warning about serious side effects of laxatives if not used according to the label or when used in the presence of certain comorbities. Sodium phosphate laxatives, according to the label, are to be taken as a single daily dose, and for no more than three days. In addition to the warning to contact a physician if the patient has kidney disease, cardiac conditions, or dehydration, the FDA advises patients to ask their physician before taking the drug with age older than 55, or when taking certain medications. These medications include: diuretics, angiotensin-converting (ACE) inhibitors, angiotensin receptor blockers (ARBs), and nonsteroidal anti-inflammatory drugs (NSAIDs).
Laxatives are grouped into different classes and have varied effects on a person's gastrointestinal system. The following is adapted from the Mayo Clinic's website and describes the main types of laxatives.
| Laxative Type
|
Action
|
Brand Example |
| Oral osmotics | Draw water into the colon to improve passage of stool | Miralax |
| Oral bulk formers | Absorb water to form soft, bulky stool | Metamucil |
| Oral stool softeners | Add moisture to stool | Surfak |
| Oral stimulants | Trigger rhythmic contractions of intestinal wall | Senekot |
| Rectal stimulants | Trigger rhythmic contractions of intestinal wall | Dulcolax |
Because laxatives can interact with medications, asking about medication lists (including supplements and herbals) is important for pelvic rehabilitation providers. Even the teas available at the grocery store that are marketed to help with digestion and specifically, constipation, may work well and may interact with a patient's medications. If you are interested in learning more about laxatives, constipation, and promotion of bowel health with rehabilitation techniques, sign up for the Bowel Pathology and Function continuing education course. This course, written by faculty member Lila Abbate, has been well-received and aims to further the knowledge of therapists who are treating patients with bowel dysfunction. The next course is coming up next month in California!
All Upcoming Continuing Education Courses


Pelvic Function Level 1 - Satellite - Fairfax VA - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026

Pelvic Function Level 1 - Satellite - Queens NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026


Pelvic Function Level 1 - Satellite - Knoxville TN - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026

Pelvic Function Level 1 - Satellite - Detroit MI - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026

Pelvic Function Level 1 - Satellite - Greenwich Village NY - February 7 - 8 2026 - SOLD OUT
Feb 7 2026 - Feb 8 2026



Pelvic Function Level 2B - Satellite - Seattle WA - February 14 - 15 2026 - SOLD OUT
Feb 14 2026 - Feb 15 2026

Pelvic Function Level 2B - Satellite - Galloway NJ - February 14 - 15 2026
Feb 14 2026 - Feb 15 2026

Pelvic Function Level 2B - Satellite - Owensboro KY - February 14 - 15 2026
Feb 14 2026 - Feb 15 2026

Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Torrance CA - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Lake Stevens WA - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026

Mobilization of Visceral Fascia: Urinary - Satellite Lab Course - Medford OR - February 20 - 22 2026
Feb 20 2026 - Feb 22 2026



Pelvic Function Level 1 - Satellite - Nashville TN - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026

Pain Science for the Chronic Pelvic Pain Population - Remote Course - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026

Pelvic Function Level 1 - In-Person - Grand Rapids MI - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026

Pelvic Function Level 1 - Satellite - Las Vegas NV - February 21 - 22 2026
Feb 21 2026 - Feb 22 2026





Pelvic Function Level 2B - In-Person - Rochester MN - February 28 - March 1 2026 - SOLD OUT
Feb 28 2026 - Mar 1 2026

Pelvic Function Level 1 - In-Person - Boston MA - February 28 - March 1 2026
Feb 28 2026 - Mar 1 2026

Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - February 28 - March 1 2026
Feb 28 2026 - Mar 1 2026

Menopause Transitions and Pelvic Rehab - Remote Course - February 28 - March 1 2026
Feb 28 2026 - Mar 1 2026

Boundaries Self-Care and Meditation - Remote Course - February 28 - March 1 2026
Feb 28 2026 - Mar 1 2026


Nutrition Perspectives for the Pelvic Rehab Therapist - Remote Course - March 7 - 8 2026
Mar 7 2026 - Mar 8 2026

Pelvic Function Level 1 - Satellite - Long Beach CA - March 7 - 8 2026 - SOLD OUT
Mar 7 2026 - Mar 8 2026


Pelvic Function Level 1 - Satellite - Fort Worth TX - March 7 - 8 2026 - SOLD OUT
Mar 7 2026 - Mar 8 2026


