
At the peak of my racing career I won awards in all my races from 5k to marathon. While warming up I would scope out my competition, intimidated by muscular females wearing outfits to accentuate their physiques. Many times, appearance out-weighed running capacity. In a similar manner, one strong pelvic floor contraction produced by a female athlete does not always mean she has the endurance to stay dry in the long run.
 Brennand et al. (2017) researched urinary leakage during exercise in Canadian women. A summary of their findings concluded that skipping, trampoline, jumping jacks, and running/jogging were most likely to cause leakage. To combat the problem, 93.2% emptied their bladder just before exercise, 62.7% required voiding breaks during exercise, and 37.3% actually restricted their fluid intake to minimize leakage. While 90.3% of women who reported leakage impacted their activity just decreased their intensity, 80.7% avoided the activity entirely. Many women used pads (49.2%). Interest in pelvic floor physiotherapy to improve their UI was high (84.6%), but 63.5% of women still sought pessary or surgical management. Unfortunately, 35.6% of the women had no idea treatment was even an option.
Brennand et al. (2017) researched urinary leakage during exercise in Canadian women. A summary of their findings concluded that skipping, trampoline, jumping jacks, and running/jogging were most likely to cause leakage. To combat the problem, 93.2% emptied their bladder just before exercise, 62.7% required voiding breaks during exercise, and 37.3% actually restricted their fluid intake to minimize leakage. While 90.3% of women who reported leakage impacted their activity just decreased their intensity, 80.7% avoided the activity entirely. Many women used pads (49.2%). Interest in pelvic floor physiotherapy to improve their UI was high (84.6%), but 63.5% of women still sought pessary or surgical management. Unfortunately, 35.6% of the women had no idea treatment was even an option.
Nygaard & Shaw (2016) reviewed and summarized the cross-sectional studies regarding the association between physical activity and pelvic floor disorders. Trampolinists, especially those in the 3rd tertile of competition, even those who were nulliparous, experienced greater leakage. Competitive athletes in the highest quartile of time exercising were found to have 2.5 times the amount of urinary incontinence (UI) as the lowest inactive quartile; however, 2nd and 3rd quartile recreational athletes had no difference in UI compared to inactive women. Type and dosage of exercise were both factors in UI risk. Various studies showed habitual walking decreased UI in older women, moderate exercise decreased the risk of UI, and no exercise increased the risk of UI. The incidence of UI being related to having performed strenuous exercise early in life has been limited and variable, with one study of Norwegian athletes and US Olympians not having any greater UI later in life, while another showed middle-aged women who used to exercise 7.5 hours per week had a higher incidence of UI. This review also reported athletes had a 20% greater cross sectional area of the levator ani muscle and a greater pubovisceral muscle mean diameter; however, the pelvic floor strength recorded was lower than non-athletes.
Interestingly, Leitner et al. (2017) explored pelvic floor muscle activation for continent and incontinent females during running. For 10 seconds, EMG tripolar vaginal probe recorded activity at 7, 11, and 15km/h. No statistically significant differences between continent or incontinent subjects were found for the EMG values. Pre-activity and reflex activity mean EMG increased significantly with speed; mean pelvic floor muscle EMG activity during running was significantly above onset activation value; and, maximum voluntary contraction was exceeded 100% for all time intervals at 15km/h in women with UI. These authors suggested the stimulus of running could actually be beneficial in pelvic floor muscle training considering the reflex activity of the muscles.
At races now, I still silently survey my competition, but now I am more curious as to how many women are actually able to complete the run without leakage. The prevalence of UI among athletes continues and is becoming more of an open topic of conversation. The research as to how much and which kind of exercise correlates with UI or what activity and level of participation may be preventative for UI is growing. The need for pelvic floor therapists to treat athletes who are fit to be dry is ever increasing.
Brennand, E., Ruiz-Mirazo, E., Tang, S., Kim-Fine, S., Calgary Women’s Pelvic Health Research Group. (2017). Urinary leakage during exercise: problematic activities, adaptive behaviors, and interest in treatment for physically active Canadian women. International Urogynecology Journal. http://www.doi:10.1007/s00192-017-3409-1
Nygaard, I. E., & Shaw, J. M. (2016). Physical Activity and the Pelvic Floor. American Journal of Obstetrics and Gynecology, 214(2), 164–171. http://doi.org/10.1016/j.ajog.2015.08.067
Leitner M, Moser H, Eichelberger P, Kuhn A, Radlinger L. (2017). Evaluation of pelvic floor muscle activity during running in continent and incontinent women: An exploratory study. Neurourology and Urodynamics. 36:1570–1576. https://doi.org/10.1002/nau.23151

You wouldn't place a newborn in a crib without knowing the legs were firmly attached at the right angle to the base. You wouldn't jump on a hammock if the poles or trees were not firmly intact and upright to support the sling. Why would you treat a pregnant woman without checking if her hips were working optimally in proper alignment to support the pelvis, inside which a new life is developing? Let's hope higher level clinicians spend the extra effort to learn about the surrounding areas that affect our specialty, whether it is pelvic floor or spine or sports medicine.
 In 2015, Branco et al., published a study entitled, “Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum.” Eleven pregnant women voluntarily participated in this descriptive longitudinal study. Ground reaction forces (GRF), joint moments of force in the sagittal, frontal, and transverse planes, and joint power in those same 3 planes were measured and assessed during gait over the course of the first, second, and third trimesters as well as 6 months post-partum. The authors found pregnancy does influence the kinetic variables of all the lower extremity joints; however, the hip joint experiences the most notable changes. As pregnancy progressed, a decrease in the mechanical load was found, with a decrease in the GRF and sagittal plane joint moments and joint powers. The vertical GRF showed the peaks of braking propulsion decreases from late pregnancy to the postpartum period. A significant reduction of hip extensor activity during loading response was detected in the sagittal plane. Ultimately, throughout pregnancy, physical activity needs to be performed in order to develop or maintain stability of the body via the lower quarter, particularly the hips.
In 2015, Branco et al., published a study entitled, “Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum.” Eleven pregnant women voluntarily participated in this descriptive longitudinal study. Ground reaction forces (GRF), joint moments of force in the sagittal, frontal, and transverse planes, and joint power in those same 3 planes were measured and assessed during gait over the course of the first, second, and third trimesters as well as 6 months post-partum. The authors found pregnancy does influence the kinetic variables of all the lower extremity joints; however, the hip joint experiences the most notable changes. As pregnancy progressed, a decrease in the mechanical load was found, with a decrease in the GRF and sagittal plane joint moments and joint powers. The vertical GRF showed the peaks of braking propulsion decreases from late pregnancy to the postpartum period. A significant reduction of hip extensor activity during loading response was detected in the sagittal plane. Ultimately, throughout pregnancy, physical activity needs to be performed in order to develop or maintain stability of the body via the lower quarter, particularly the hips.
The same authors, in 2013, studied gait analysis in the second and third trimesters of pregnancy. Branco et al., performed a 3-dimensional gait analysis of 22 pregnant women and 12 non-pregnant women to discern kinetic differences in the groups. Nineteen dependent variables were measured, and no change was noted between 2nd and 3rd trimesters or the control group for walking speed, stride width, right-/left-step time, cycle time and time of support, or flight phases. Comparing the 2nd versus 3rd trimester, a decrease in stride and right-/left-step lengths decreased. The 2nd and 3rd trimesters both showed a significant decrease in right hip extension and adduction during the stance phase when compared to the control group. In this study, the authors also noted increased left knee flexion and decreased right ankle plantar flexion during gait from the 2nd to the 3rd trimester. The bottom line in this study, just as the more recent one suggests, pregnant women need a higher degree of lower quarter stability to ambulate efficiently throughout pregnancy.
Physical therapists are movement specialists with a unique opportunity to analyze how humans function, whether athletes or pregnant women (or even a pregnant athlete). How the hips move and whether or not proper muscles are firing can affect anyone’s gait. The extra demands on the pregnant body require more specific analysis of kinetics by therapists, thus directing the protocols for rehabilitation of this population. It should behoove every pelvic floor specialist, in particular, to attend a course like “Biomechanical Assessment of the Hip and Pelvis" or "Care of the Pregnant Patient" in order to provide patients with the optimal support for the natural “crib” women provide during pregnancy.
Branco, M., Santos-Rocha, R., Vieira, F., Aguiar, L., & Veloso, A. P. (2015). Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum. Scientifica, 2015, 580374. http://doi.org/10.1155/2015/580374
Branco, M., Santos-Rocha, R., Aguiar, L., Vieira, F., & Veloso, A. (2013). Kinematic Analysis of Gait in the Second and Third Trimesters of Pregnancy.Journal of Pregnancy, 2013, 718095. http://doi.org/10.1155/2013/718095

Nancy Cullinane PT, MHS, WCS is today's guest blogger. Nancy has been practicing pelvic rehabilitation since 1994 and she is eager to share her knowledge with the medical community at large. Thank you, Nancy, for contributing this excellent article!
Clinically valid research on the efficacy and safety of therapeutic exercise and activities for individuals with osteoporosis or vertebral fractures is scarce, posing barriers for health care providers and patients seeking to utilize exercise as a means to improve function or reduce fracture risk1,2. However, what evidence does exist strongly supports the use of exercise for the treatment of low Bone Mineral Density (BMD), thoracic kyphosis, and fall risk reduction, three themes that connect repeatedly in the body of literature addressing osteoporosis intervention.
Sinaki et al3 reported that osteoporotic women who participated in a prone back extensor strength exercise routine for 2 years experienced vertebral compression fracture at a 1% rate, while a control group experienced fracture rates of 4%. Back strength was significantly higher in the exercise group and at 10 years, the exercise group had lost 16% of their baseline strength, while the control group had lost 27%. In another study, Hongo correlated decreased back muscle strength with an increased thoracic kyphosis, which is associated with more fractures and less quality of life. Greater spine strength correlated to greater BMD4. Likewise, Mika reported that kyphosis deformity was more related to muscle weakness than to reduced BMD5. While strength is clearly a priority in choosing therapeutic exercise for this population, fall and fracture prevention is a critical component of treatment for them as well. Liu-Ambrose identified quadricep muscle weakness and balance deficit statistically more likely in an osteoporotic group versus non osteoporotics6. In a different study, Liu-Ambrose demonstrated exercise-induced reductions in fall risk that were maintained in older women following three different types of exercise over a six month timeframe. Fall risk was 43% lower in a resistance-exercise training group; 40% lower in a balance training exercise group, and 37% less in a general stretching exercise group7.
These studies allow us to unequivocally conclude that spinal extensor strengthening and therapeutic activities aimed at improving balance and decreasing fall risk are tantamount as therapeutic interventions for osteoporosis. But postural education/modification and weight bearing activities aimed at stimulating osteoblast production intended to improve BMD are a reasonable component of an osteoporosis treatment plan, despite the lack of concrete evidence for them. Nutrition and mineral supplementation with calcium and vitamin D have been shown to reduce morbidities, and hence we should incorporate this education into our treatment plans as well8, 9. Studies on the efficacy of vibration platforms hold promise, but thus far, have not been substantiated as an evidence-based intervention to improve BMD.
Too Fit To Fracture: outcomes of a Delphi consensus process on physical activity and exercise recommendations for adults with osteoporosis with or without vertebral fractures1,2 is a multiple-part publication in the journal Osteoporosis International, based upon an international consensus process by expert researchers and clinicians in the osteoporosis field. These publications include exercise and physical activity recommendations for individuals with osteoporosis based upon a separation of patients into to three groups: osteoporosis based on BMD without fracture; osteoporosis with one vertebral fracture; and osteoporosis with multiple spine fractures, hyperkyphosis and pain. This group of experts emphasize the importance of teaching safe performance of ADLs with respect to bodymechanics as a priority to accompany strength, balance, fall & fracture prevention, nutrition and pharmacotherapy management. They promote establishment of an individualized program for each patient with adaptable variations of these concepts, with the most accommodation allotted for individuals with multiple vertebral compression fractures. An example of such an adaptation is altering prone back extensions such as those documented in the studies by Sinaki and Hongo, into supine shoulder presses, thus strengthening the back extensors in a less gravitationally demanding posture. Osteoporosis Canada has adapted the main concepts from these publications into a patient-friendly, instructional website with reproducible handouts at http://www.osteoporosis.ca/osteoporosis-and-you/too-fit-to-fracture/
A firm conclusion from the Too Fit to Fracture project is that higher quality outcomes studies are desperately needed to assist all healthcare providers in managing osteoporosis more effectively and comprehensively, and to do so prior to the onset of debilitating fractures that tend to produce serious comorbidities.
1. Giangregorio et al. Too Fit to Fracture: exercise recommendations for individuals with osteoporosis or osteoporotic vertebral fracture. Osteoporosis International. 2014; 25(3): 821-835
2. Giangregorio et al. Too Fit to Fracture: outcomes of a Delphi consensus process on physical activity and exercise recommendations for adults with osteoporosis with or without vertebral fracture. Osteoporosis International. 2015; 26(3):891-910
3. Sinaki et al. Stronger back muscles reduce the incidence of vertebral fractures: a prospective 10 year follow-up of postmenopausal women. Bone. 2002; 30: 836-841 4. Hongo et al. Effect of low-intensity back exercise on quality of life and back extensor strength in patients with osteoporosis; a randomized controlled trial.Osteoporosis International. 2007; 10: 1389-1395
5. Mika et al. Differences in thoracic kyphosis and in back muscle strength in women with bone loss due to osteoporosis. Spine. 2005; 30(2): 241-246
6. Liu-Ambrose et al. Older women with osteoporosis have increased postural sway and weaker quadriceps strength than counterparts with normal bone mass: overlooked determinants of fracture risk? J Gerontology, Series A Biolog Sci Med Sci. 2003; 58(9): M862-866
7. Liu-Ambrose et al. The beneficial effects of group-based exercise on fall risk profile and physical activity persist 1 year post intervention in older women with low bone mass: follow-up after withdrawal of exercise. J Am Geriat Soc. 2005; 53 (10): 1767-1773
8. Ensrud et al. Weight change and fractures in older women: study of osteoporotic fractures research group. Archives Int Med. 1997; 157 (8): 857-863
9. Kemmler et al. Exercise effects on fitness and bone mineral density in early postmenopausal women: 1-year EFOPS results. Med and Sci in Sports Ex. 2002; 34 (12): 2115-2123
Dr. Dischiavi is a Herman & Wallace faculty member who authored and teaches Biomechanical Assessment of the Hip & Pelvis: Manual Movement Therapy and the Myofascial Sling System, available this August in Boston, MA.
STEM is an acronym for science, technology, engineering, and math. These fields are deeply intertwined and taking this approach could potentially be a way to facilitate the physical therapist’s appreciation of human movement.
 Science: I would bet most physical therapists would agree that science is the cornerstone of our profession. It is time to look across all the landscapes of science to better understand the physical principles that govern movement. Biotensegrity is a great example of how science from a field such as cellular biology can help possibly explain how we maintain an erect posture when the rigid bony structure of our skeleton is only connected from bone to bone by soft tissues [1]. The brain and central nervous system regulates muscle tone, and it is resting muscle tone that give our bodies the ability to be upright. Without resting muscle tone, we would crumple to the ground as a heap of bones within a bag of skin. Since the CNS can either up or down regulate muscle tone, this allows us to create the rigidity we need to accomplish higher level movements such as sport, and then return to a resting state after the movements are performed (see running skeleton picture below). This theory of organismic support was bred within the scientific field of cellular biology, and can potentially be applied effectively to the human organism. As physical therapists, I agree we need to be skeptical of new ideas, but we also need to embrace the idea that the physical sciences have applied to nature for centuries, and it is possible these various scientific fields can help us unlock new ideas and allow us to look at things through a different lens.
Science: I would bet most physical therapists would agree that science is the cornerstone of our profession. It is time to look across all the landscapes of science to better understand the physical principles that govern movement. Biotensegrity is a great example of how science from a field such as cellular biology can help possibly explain how we maintain an erect posture when the rigid bony structure of our skeleton is only connected from bone to bone by soft tissues [1]. The brain and central nervous system regulates muscle tone, and it is resting muscle tone that give our bodies the ability to be upright. Without resting muscle tone, we would crumple to the ground as a heap of bones within a bag of skin. Since the CNS can either up or down regulate muscle tone, this allows us to create the rigidity we need to accomplish higher level movements such as sport, and then return to a resting state after the movements are performed (see running skeleton picture below). This theory of organismic support was bred within the scientific field of cellular biology, and can potentially be applied effectively to the human organism. As physical therapists, I agree we need to be skeptical of new ideas, but we also need to embrace the idea that the physical sciences have applied to nature for centuries, and it is possible these various scientific fields can help us unlock new ideas and allow us to look at things through a different lens.
 Technology: As not only a practicing physical therapist, but as a newly appointed assistant professor within a budding physical therapy program it is my duty to embrace evidence based practice. I believe without question, when evidence that is sound exists it should help direct patient care. It is also clear that our tests and measures that are currently being utilized to help develop new evidence are lacking, specifically with regard to human movement and sport performance.
Technology: As not only a practicing physical therapist, but as a newly appointed assistant professor within a budding physical therapy program it is my duty to embrace evidence based practice. I believe without question, when evidence that is sound exists it should help direct patient care. It is also clear that our tests and measures that are currently being utilized to help develop new evidence are lacking, specifically with regard to human movement and sport performance.
Sports performance is such a complex system (more on this later) we can’t expect to study things such as injury prevention at slow speeds utilizing maneuvers that aren’t even seen in the sport itself. Recently, Bahr [2] suggested that screening for sports injuries is pretty much a futile effort as he titled his article “Why screening tests to predict injury do not work - and probably never will…: a critical review.” Eventually technology will need to be developed that can measure high speed movement across multiple planes and ranges of motion, and essentially capture the complex spiraling that occurs with human movement and the bodies effort to attenuate ground reaction forces. This concept can be illustrated in the current work of Tak and Langhout [3] who have developed a novel approach to measure hip ROM in soccer players. They have essentially performed a thorough needs analysis of the kicking motion and determined that the classical method of measuring hip ROM doesn’t take into account the body’s need to spiral itself to gain the energy in the system needed to kick a ball [Fig 1]. This global understanding of the dynamic integration of the kinetic chain (which is covered in my hip course!) is what has led them to design this new method to measure hip ROM. Now, we will need technological advancements to capture, record, and measure these types of positions across three planes and at high speeds to establish the data that will eventually lead to evidence that will translate into sport. This is a great example of how clinical innovation sometimes precedes actual evidence to support its use. As William Blake was quoted as saying “what is now proven was once only imagined.”
 Engineering: Structural engineering should be included in every physical therapy education program. There are many basic structural engineering principles that directly apply to a physical therapists practice. For example, the principal of elastics is frequently discussed within structural engineering. Elastics describes to what extent deformation is proportional to the forces applied to a particular material. In physical therapy muscles are that particular material, muscles must have elasticity and extensibility, not flexibility! In elastics, a rubber band is often used as a simple example to explain this engineering concept.
Engineering: Structural engineering should be included in every physical therapy education program. There are many basic structural engineering principles that directly apply to a physical therapists practice. For example, the principal of elastics is frequently discussed within structural engineering. Elastics describes to what extent deformation is proportional to the forces applied to a particular material. In physical therapy muscles are that particular material, muscles must have elasticity and extensibility, not flexibility! In elastics, a rubber band is often used as a simple example to explain this engineering concept.
A rubber band will elongate and develop potential energy until release and then unleash kinetic energy. Our human movement system relies heavily on the principle of elastics. The rectus femoris is a two-joint muscle across the hip. During gait and running the rectus femoris is elongated as the hip moves into extension, this elongation builds its potential energy until the foot comes off the ground to initiate the swing phase, and the kinetic energy released in the system allows momentum to carry the lower extremity forward.
 I would add that possibly the twisting created by the contralateral counter trunk rotation and reciprocating arm and leg swing that accompanies the hip extension is what creates tension throughout the entire anterior chain, similar to why Tak and Langhout feel its important to take up all soft tissue slack three dimensionally to effectively measure hip ROM needed for a soccer kick. It is considering that the elasticity in the entire system (organism) is needed to create an efficient human movement, which is kicking a ball in this example. When the body utilizes passive lengthening of muscle chains, as in elastics, it allows the body to move more efficiently. This is described by Chu [4] who reports that in the pitching motion maximizing force development in the large muscles of the core and legs produces more than 51%- 55% of the kinetic energy that is transferred to the hand [Fig 2]. The thoracolumbar fascia is involved in the kinetic chain during throwing activities and connects the lower limbs through the gluteus maximus muscle to the upper limbs through the latissimus dorsi. This idea of a dynamic integration of the kinetic chain is the main concept of the exercise portion of my hip course!
I would add that possibly the twisting created by the contralateral counter trunk rotation and reciprocating arm and leg swing that accompanies the hip extension is what creates tension throughout the entire anterior chain, similar to why Tak and Langhout feel its important to take up all soft tissue slack three dimensionally to effectively measure hip ROM needed for a soccer kick. It is considering that the elasticity in the entire system (organism) is needed to create an efficient human movement, which is kicking a ball in this example. When the body utilizes passive lengthening of muscle chains, as in elastics, it allows the body to move more efficiently. This is described by Chu [4] who reports that in the pitching motion maximizing force development in the large muscles of the core and legs produces more than 51%- 55% of the kinetic energy that is transferred to the hand [Fig 2]. The thoracolumbar fascia is involved in the kinetic chain during throwing activities and connects the lower limbs through the gluteus maximus muscle to the upper limbs through the latissimus dorsi. This idea of a dynamic integration of the kinetic chain is the main concept of the exercise portion of my hip course!
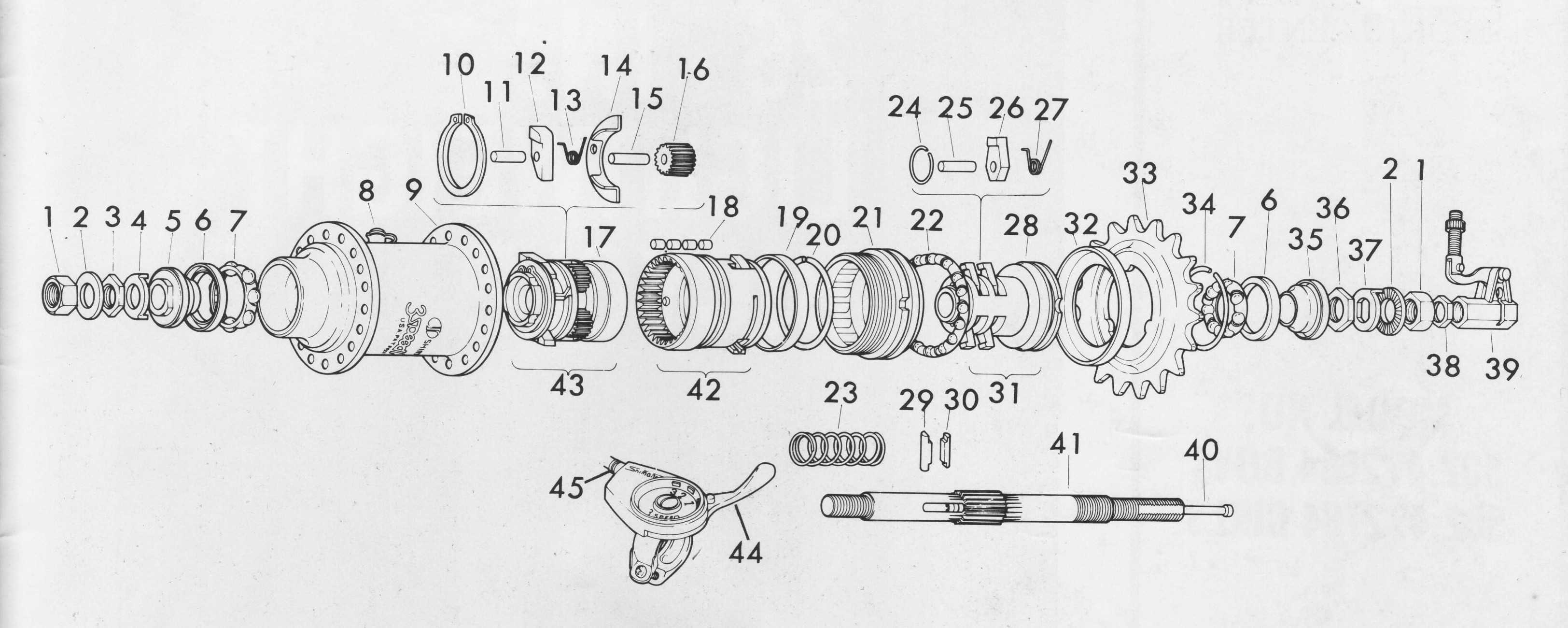
 Math: The dynamic systems theory is an area of mathematics that most physical therapists probably don’t consider during everyday treatment. Little do they know, every treatment decision we as therapists make for our patient/clients has some root found in the dynamic systems theory. In fact, it is a fitting description when this theory is applied to human movement. Human movement is an incredibly complex system comprised of many different systems all working at the same time. Paul Glazier recently offered a Grand Unified Theory (GUT) for sports performance [5] and he discusses in detail the various systems and dynamic elements involved in sports performance from musculoskeletal, to neural, to cognitive, environmental, hormonal, and emotional just to name a few. The systems at work during sport when combined are exponential and most likely infinite. This is why it is so difficult to try and capture all these dynamic systems in a laboratory setting with the current technology available. In my hip course offered through Herman & Wallace I offer a novel paradigm to help clinicians construct therapeutic exercise programs using the hip as a cornerstone to human movement. I try to compact these various systems into 8 overlapping elements related to sport performance. When each of these 8 components are “exploded” as you might see in an engineering schematic where an engine is exploded to see all the parts that make the engine or more simply explained using a cheeseburger as the example [Fig 3]. Sure its easy to spot the cheeseburger when its whole just like when you see an athlete on the field running it seems obvious. Once the cheeseburger is “exploded” you can now isolate each sub-element included in your cheeseburger. This cheeseburger example is an obvious over-simplification, but if we exploded the bun to see the underlying grain and the seeds and so on…you now start to get an idea of how deep and intertwined all these subsystems are. Interestingly, the engine and the cheeseburger have finite parts and fit together, the human system has different parts in different systems depending on the sport and who might be playing it, under ever-changing scenery, and so on. So you can now see how the 8 components I outline in my course can house many different aspects of these dynamic systems. Although, I think this is progress with regard to the current state of the evidence, specifically with regard to utilizing the hip during movement, there are other systems at work that clinicians simply cannot control, such as gender, hormonal, environmental, etc…The idea is to try to identify and then manipulate modifiable factors whenever possible. These concepts are more clearly described and implemented in my hip course! Please come and check it out, and let me know what you think!
Math: The dynamic systems theory is an area of mathematics that most physical therapists probably don’t consider during everyday treatment. Little do they know, every treatment decision we as therapists make for our patient/clients has some root found in the dynamic systems theory. In fact, it is a fitting description when this theory is applied to human movement. Human movement is an incredibly complex system comprised of many different systems all working at the same time. Paul Glazier recently offered a Grand Unified Theory (GUT) for sports performance [5] and he discusses in detail the various systems and dynamic elements involved in sports performance from musculoskeletal, to neural, to cognitive, environmental, hormonal, and emotional just to name a few. The systems at work during sport when combined are exponential and most likely infinite. This is why it is so difficult to try and capture all these dynamic systems in a laboratory setting with the current technology available. In my hip course offered through Herman & Wallace I offer a novel paradigm to help clinicians construct therapeutic exercise programs using the hip as a cornerstone to human movement. I try to compact these various systems into 8 overlapping elements related to sport performance. When each of these 8 components are “exploded” as you might see in an engineering schematic where an engine is exploded to see all the parts that make the engine or more simply explained using a cheeseburger as the example [Fig 3]. Sure its easy to spot the cheeseburger when its whole just like when you see an athlete on the field running it seems obvious. Once the cheeseburger is “exploded” you can now isolate each sub-element included in your cheeseburger. This cheeseburger example is an obvious over-simplification, but if we exploded the bun to see the underlying grain and the seeds and so on…you now start to get an idea of how deep and intertwined all these subsystems are. Interestingly, the engine and the cheeseburger have finite parts and fit together, the human system has different parts in different systems depending on the sport and who might be playing it, under ever-changing scenery, and so on. So you can now see how the 8 components I outline in my course can house many different aspects of these dynamic systems. Although, I think this is progress with regard to the current state of the evidence, specifically with regard to utilizing the hip during movement, there are other systems at work that clinicians simply cannot control, such as gender, hormonal, environmental, etc…The idea is to try to identify and then manipulate modifiable factors whenever possible. These concepts are more clearly described and implemented in my hip course! Please come and check it out, and let me know what you think!
I’m hoping the STEM approach can possibly make it into physical therapy curriculums to illustrate to future physical therapists that there are many different disciplines at work with regard to physical therapy, and taking a global view of these elements can certainly be worthwhile.
1. Ingber, D.E., N. Wang, and D. Stamenovic, Tensegrity, cellular biophysics, and the mechanics of living systems. Rep Prog Phys, 2014. 77(4): p. 046603.
2. Bahr, R., Why screening tests to predict injury do not work-and probably never will...: a critical review. Br J Sports Med, 2016.
3. Tak, I., et al., Hip Range of Motion Is Lower in Professional Soccer Players With Hip and Groin Symptoms or Previous Injuries, Independent of Cam Deformities. Am J Sports Med, 2016. 44(3): p. 682-8.
4. Chu, S.K., et al., The Kinetic Chain Revisited: New Concepts on Throwing Mechanics and Injury. PM R, 2016. 8(3 Suppl): p. S69-77.
5. Glazier, P.S., Towards a Grand Unified Theory of sports performance. Hum Mov Sci, 2015.
Figure 1


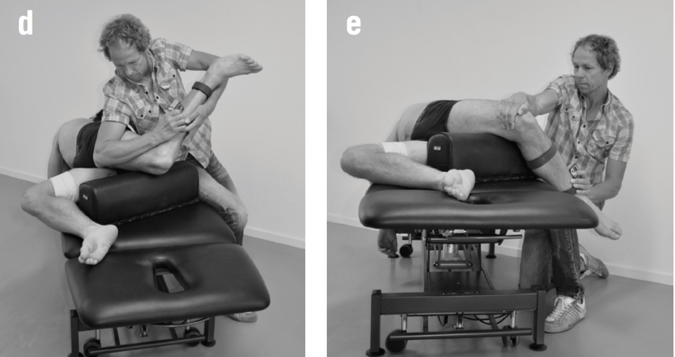
Figure 2
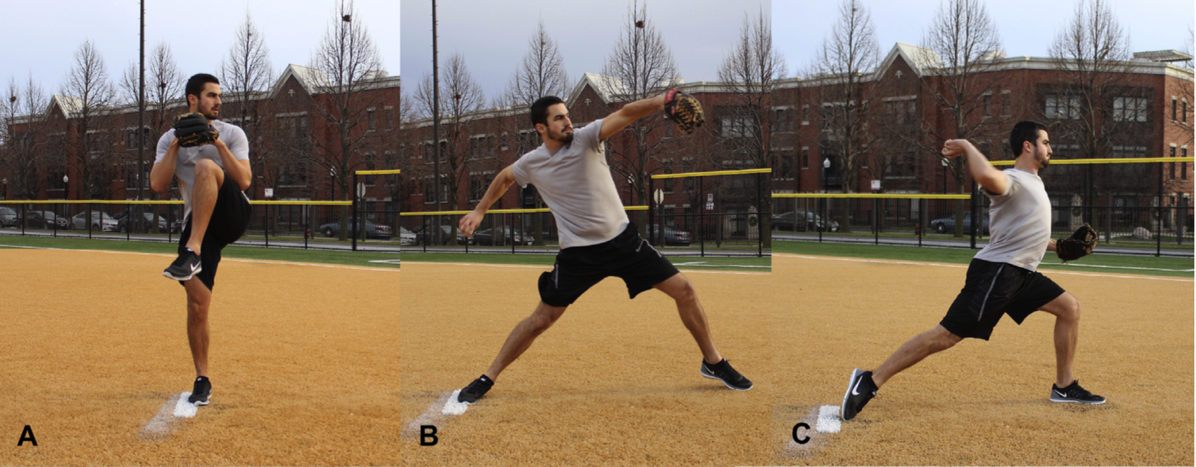
Figure 3
Figure 4

Dr. Steve Dischiavi, MPT, DPT, SCS, ATC, COMT, a Herman & Wallace faculty member, recently co-authored a peer reviewed manuscript which reviewed hip focused exercise programs. Dr. Dischiavi currently teaches a hip related course in the Herman & Wallace curriculum titled “Biomechanical Assessment of the Hip & Pelvis: Dynamic Integration of the Myofascial Sling Systems.”
 "An evidence based review of hip focused neuromuscular exercise interventions to address dynamic lower extremity valgus", published in the Journal of Sports Medicine, presents evidence related to current hip focused interventions within the physical therapy profession. We know that there has been an enormous increase in the amount of hip related diagnoses and surgeries, and this calls for better knowledge from the clinicians on how to manage these particular hip related pathologies. The review finds that insufficient research has been done "to identify and understand the mechanistic relationship between optimized biomechanics during sports and hip-focused neuromuscular exercise interventions... improved strength does not always result in changes to important biomechanical variables, and improved biomechanics in sports-related tasks does not necessarily equal improved biomechanical variables in performance of the sport itself".
"An evidence based review of hip focused neuromuscular exercise interventions to address dynamic lower extremity valgus", published in the Journal of Sports Medicine, presents evidence related to current hip focused interventions within the physical therapy profession. We know that there has been an enormous increase in the amount of hip related diagnoses and surgeries, and this calls for better knowledge from the clinicians on how to manage these particular hip related pathologies. The review finds that insufficient research has been done "to identify and understand the mechanistic relationship between optimized biomechanics during sports and hip-focused neuromuscular exercise interventions... improved strength does not always result in changes to important biomechanical variables, and improved biomechanics in sports-related tasks does not necessarily equal improved biomechanical variables in performance of the sport itself".
Biomechanical Assessment of the Hip & Pelvis is an opportunity to explore manual movement therapy with a skilled researcher and practitioner. Dr. Dischiavi has woven a very creative and innovative philosophy to help clinicians design more comprehensive hip focused therapeutic interventions. His in-depth knowledge of the evidence has allowed him to create a program that will challenge clinicians in new ways to look at the hip, pelvis, and lower extremity and how the kinetic chain can be influenced by approaching it using a new lens.
Participants of his course will learn new ways to activate and strengthen groups of pelvic muscles that will benefit all patients from pelvic health clients, to professional athletes, to your elderly population. “All patients have the same bones, muscles, and gravitational pulls acting on them, its how they use these systems that varies significantly. A philosophical science can be generated, but the art is in implementing that science.”
Participants in the Biomechanical Assessment of the Hip & Pelvis course have enjoyed being challenged to look at the hip and pelvis in a different way. Practitioners will leave the course having learned a whole new way to develop and implement therapeutic exercises which are a different approach from the single plane non-weight bearing exercises that are traditionally prescribed to patients.
There are many courses and philosophies on how to screen for lower extremity injuries and how to evaluate movement dysfunction. What is really lacking for clinicians are options for therapeutic exercises which target the hip and pelvis in a relevant and functional manner. Most hip focused programs currently emphasize single plane movements and are dominated with concentric focused exercise. Dr. Dischiavi’s focus is targeted directly at human movement emphasizing tri-planar movements that are primarily eccentric in nature, recognizing that this is how the human body functions.
Come to the Biomechanical Assessment of the Hip & Pelvis: Manual Movement Therapy and the Myofascial Sling System in Seattle this June, or in Boston this August!
Herman & Wallace faculty member Eric Dinkins, PT, MS, OCS, Cert. MT, MCTA teaches the Manual Therapy for the Lumbo-Pelvic-Hip Complex: Mobilization with Movement and Laser-Guided Feedback for Core Stabilization course for Herman & Wallace. He is one of only 13 practitioners in America credentialed to teach the Mulligan Concept of Manual Therapy, and is a published author. Join him in Arlington, VA on August 20-21, 2016 to learn new joint mobilization, evaluation, and treatment skills.
Much research has been published regarding evaluation and diagnosis of the Sacroiliac Joint (SIJ). Low back pain and pelvic girdle pain is a common complaint with patients in all clinic settings. Laslett (Manual Therapy 2005) gave our profession valuable insight into categorizing a cluster of tests to try to ensure Physical Therapists and Chiropractors know if the SI joint is a pain source of our patients. We now also have several articles reaffirming the validity of the Active Straight Leg Raise (ASLR) and Stork testing for SIJ dysfunction (Manual Therapy 2008; JBMR 2012; PT 2007). However, after talking with clinicians who attend my Mobilization with Movement classes, as well as many colleagues in the outpatient orthopedic setting, there is a definitive lack of understanding how to use this information to translate over to successful treatment. This is understandable considering there have been several articles published regarding the poor validity and consistency between clinicians regarding palpation skills and bony landmarks in the lumbar spine and pelvis (ex: Manual Therapy 2012). But perhaps the fault is not in the clinician proficiency, but rather in the nature that we are attempting to diagnose an SIJ dysfunction?
 If you were to consult with experts in body kinematics, gait analysis, and biomechanics regarding the true movement of the SIJ, there will be many different answers depending on the action that they were describing. Particularly when it comes to dysfunction. Disagreements abound when describing conditions such as “upslips”, “inflares”, etc and virtually all back their arguments with clinical anecdotal success rates. These arguments often leave clinicians with inconsistencies in treatment and increased failures.
If you were to consult with experts in body kinematics, gait analysis, and biomechanics regarding the true movement of the SIJ, there will be many different answers depending on the action that they were describing. Particularly when it comes to dysfunction. Disagreements abound when describing conditions such as “upslips”, “inflares”, etc and virtually all back their arguments with clinical anecdotal success rates. These arguments often leave clinicians with inconsistencies in treatment and increased failures.
This blog is meant to be a persuasive argument for using function-improving or pain- eliminating techniques for diagnosis and treatment of SIJ dysfunction. The logic of this approach is often misunderstood. But if applied correctly, satisfies most theory surrounding the SIJ, and provides immediate feedback for knowing how to resolve the condition and what you are treating.
We have pain provocative testing that is most commonly used in attempting to diagnose a SIJ dysfunction. However, after interpreting these tests, the clinician is still left without a true diagnosis as to the nature of what is happening at this joint to cause pain or dysfunction. This is likened to the "painful shoulder" or "low back pain" prescription we see. The error rates, even in the cluster, still leaves room for inaccurate assessment and therefore potential misguided treatment. Lumbar facet, musculature, hip capsule imbalance, are just some examples that can produce false positives on the typical SIJ tests that are used in clinic. Therefore, it is necessary to understand that pain provocative testing ONLY tells us that pain is coming from that structure that is being tested. And NOT that it is “THE” source of the dysfunction.
Now consider using function-improving or pain-eliminating techniques for your evaluation. The ALSR test, as an example, function improving special test. Compression applied to various aspects of the pelvis or supporting musculature yield a positive finding if the SLR is now easier if the force is applied. Combing this information with the faulty kinetic testing of the Stork and/or leg pull test to determine the involved side yield an immediate feedback for both the clinician and the patient as to what forces are needed to correct the dysfunction that is limiting the functional activity and restore normal motion. Treatment would then be applied by creating a force on the innominate, sacrum, or both and would then be maintained throughout the movement and can be considered a form of active exercise (manual assisted active exercise). If retesting of the affected motion yields a sustained improvement, the accurate diagnosis has now been made. And surely this diagnosis would be upheld if the patient returned at a later date to demonstrate no regression occurred.
If the force applied to the pelvis was directed toward posterior rotation at the innominate and/or an anterior rotation at the sacrum, and the affected motion cleared without pain or limited motion, it would be confirmed that these forces were necessary to correct the dysfunction on the involved side regardless of the "ambiguous diagnosis' including the potential of a previously held thought of an anterior rotation of the pelvis (making the argument of what actually happened at the pelvis mute). This may have been achieved through altering inputs viewed as a potential "threat" by the system, or mechanics stresses, etc. Regardless, if manual correction of this condition was applied and the dysfunction was correction through re-creating this without pain, one would conclude that this dysfunction was the primary eitiology of the symptoms. If the symptoms returned or the functional test was not normalized, an easy conclusion would then be that despite manual correction eliminating pain during the activity, this correction was not addressing the source of the dysfunction. And therefore the clinician should consider treatment elsewhere.
In essence, the body is capable of directing what it needs in order to return to a normal functioning homeostasis…without the application of pain. Now this pain-eliminating testing becomes your assessment, treatment and potentially your home exercise program!
To conclude, it is my suggestion to all manual based physiotherapists and chiropractors to strongly consider pain-eliminating techniques for both evaluation and treatment in their practice.
Did I mention yet that your patient already voted for that….?
Laslett, M, et al. "Diagnosis of Sacroiliac Joint Pain: Validity of individual provocation tests and composites of tests" Manual Therapy 10 (2005) 207-218
M. de Groot, et al. "The active straight leg raising test (ASLR) in pregnant women: Differences in muscle activity and force between patients and health subjects" Manual Therapy 13 (2008) 68-74
Hungerford, B, et al. "Evaluation of the Ability of Physical Therapists to Palpate Intrapelvic Motion with the Stork Test on the Support Side" Phys Ther. 2007 Jul;87(7):879-87.
O'Surrivan PB, Beales DJ. "Diagnosis and classification of pelvic girdle pain disorders—Part 1: A mechanism based approach within a biopsychosocial framework" Man Ther. 2007 May;12(2):86-97.
Arab AM, Abdollahi I, Joghataei MT, Golafshani Z, Kazemnejad A. "Inter- and intra-examiner reliability of single and composites of selected motion palpation and pain provocation tests for sacroiliac joint" Man Ther. 2009 Apr;14(2):213-21. doi: 10.1016/j.math.2008.02.004. Epub 2008 Mar 25.
An article appearing this year in Arthroscopy details a systematic review completed to determine if asymptomatic individuals show evidence on imaging of femoroacetabular impingement, or FAI. Cam, pincer, and combined lesions were included in the results. To read some basics about femoroacetabular injury, click here. Over 2100 hips (57% men, 43% women) with a mean age of 25 were studied. (Only seven of the 26 studies reported on labral tears.) The researchers found the following prevalence in this asymptomatic population:
Cam lesion: 37% (55% in athletes versus 23% in general population)
Pincer lesion: 67%
Labral tears: 68%
Mean lateral and anterior center edge angles: 30-31 degrees
The authors conclude that femoroacetabular impingement tissue changes and hip labral injury are common findings in asymptomatic patients, therefore, clinicians must determine the relevance of the findings in relation to patient history and physical examination. Because hip pain is a common comorbidity of pelvic pain, knowing how to screen the hip joint for FAI or labral tears, rehabilitate hips with joint dysfunction, and help someone return to activity following a hip repair is valuable to the pelvic rehabilitation therapist.
As the athletic population may have increased risk of hip injuries due to overuse, traumatic injury, or vigorous activity, being able to address dysfunction in both high level and less active patients is necessary. Herman & Wallace faculty member Steve Dischiavi has developed a course rich in athletic examples and including education about activating fascial systems in various planes. If you are ready to step up your game related to Biomechanical Assessment of the Hip & Pelvis, check out this continuing education course taking place next in Durham, North Carolina in May.
All Upcoming Continuing Education Courses

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 25 - 26 2025
Apr 25 2025 - Apr 26 2025

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025

Pelvic Function Level 1 - Satellite - Bethpage NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025


Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Pelvic Function Level 1 - Satellite - Marietta GA - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025






Biofeedback for Pelvic Muscle Dysfunction Satellite Lab Course - Self-Hosted - May 4 2025
May 4 2025





Pelvic Function Level 1 - Satellite - Plainfield IN - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025





Pelvic Function Level 1 - Satellite - Las Vegas NV - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bradenton FL - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Philadelphia PA - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Atlanta GA - May 16 - 18 2025 (Instructor Site)
May 16 2025 - May 18 2025
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bellingham WA - May 16 - 18 2025
May 16 2025 - May 18 2025





Lumbar Nerve Manual Assessment and Treatment - Remote Course - May 17 - 18 2025
May 17 2025 - May 18 2025



Pelvic Function Level 1 - Satellite - Galloway NJ - May 31 - June 1 2025 - SOLD OUT
May 31 2025 - Jun 1 2025
