
The new year is here and with it, lots of motivational posting about exercise and weight loss…but how is this desire for ‘new year, new you’ affecting peri-menopausal women with urinary dysfunction? It has been established that the lower urinary tract is sensitive to the effects of estrogen, sharing a common embryological origin with the female genital tract, the urogenital sinus. Urge urinary incontinence is more prevalent after the menopause, and the peak prevalence of stress incontinence occurs around the time of the menopause (Quinn et al 2009). Zhu et al looked at the risk factors for urinary incontinence in women and found that some of the main contributors include peri/post-menopausal status, constipation and central obesity (women's waist circumference, >/=80 cm) along with vaginal delivery/multiparity.
 Could weight loss directly impact urinary incontinence in menopausal women? In a word – yes. ‘Weight reduction is an effective treatment for overweight and obese women with UI. Weight loss of 5% to 10% has an efficacy similar to that of other nonsurgical treatments and should be considered a first line therapy for incontinence’ (Subak et al 2005) But do these benefits last? Again – yes! ‘Weight loss intervention reduced the frequency of stress incontinence episodes through 12 months and improved patient satisfaction with changes in incontinence through 18 months. Improving weight loss maintenance may provide longer term benefits for urinary incontinence.’ (Wing et al 2010)
Could weight loss directly impact urinary incontinence in menopausal women? In a word – yes. ‘Weight reduction is an effective treatment for overweight and obese women with UI. Weight loss of 5% to 10% has an efficacy similar to that of other nonsurgical treatments and should be considered a first line therapy for incontinence’ (Subak et al 2005) But do these benefits last? Again – yes! ‘Weight loss intervention reduced the frequency of stress incontinence episodes through 12 months and improved patient satisfaction with changes in incontinence through 18 months. Improving weight loss maintenance may provide longer term benefits for urinary incontinence.’ (Wing et al 2010)
The other major health issues facing women at midlife include an increased risk for cardiovascular disease, Type 2 Diabetes and Bone Health problems – all of which are responsive to lifestyle interventions, particularly exercise and stress management. In their paper looking at lifestyle weight loss interventions, Franz et al found that ‘…a weight loss of >5% appears necessary for beneficial effects on HbA1c, lipids, and blood pressure. Achieving this level of weight loss requires intense interventions, including energy restriction, regular physical activity, and frequent contact with health professionals’. 5% weight loss is the same amount of weight loss necessary to provide significant benefits for urinary incontinence at midlife.
Successful weight management depends on nutritional intake, exercise and psychosocial considerations such as stress management, but for the menopausal woman, hormonal balance can also have an effect on not only bladder and bowel dysfunction but changing metabolic rates, thyroid issues and altered weight distribution patterns. As pelvic rehab therapists, we are all aware that pelvic health issues can be a barrier to exercise participation but sensitive awareness of the other particular challenges facing midlife women can make the difference in developing a beneficial therapeutic alliance and a journey back to optimal health. If you would like to explore the topics surrounding optimal health at menopause, why not join me in California in February?
Climacteric. 2009 Apr;12(2):106-13. ‘The effects of hormones on urinary incontinence in postmenopausal women.’ Quinn SD, Domoney C. Menopause. 2009 Jul-Aug;16(4):831-6. The epidemiological study of women with urinary incontinence and risk factors for stress urinary incontinence in China’ Zhu L, Lang J, Liu C, Han S, Huang J, Li X. J Urol. 2005 Jul;174(1):190-5. Weight loss: a novel and effective treatment for urinary incontinence’ Subak LL, Whitcomb E, Shen H, Saxton J, Vittinghoff E, Brown JS. J Urol. 2010 Sep;184(3):1005-10. Effect of weight loss on urinary incontinence in overweight and obese women: results at 12 and 18 months Wing RR, West DS, Grady D, Creasman JM, Richter HE, Myers D, Burgio KL, Franklin F, Gorin AA, Vittinghoff E, Macer J, Kusek JW, Subak LL; Program to Reduce Incontinence by Diet and Exercise Group. J Acad Nutr Diet. 2015 Sep;115(9):1447-63. doi: 10.1016/j.jand.2015.02.031. Epub 2015 Apr 29. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: a systematic review and meta-analysis of randomized clinical trials. Franz MJ, Boucher JL, Rutten-Ramos S, VanWormer JJ. Lean, M, & Lara, J & O Hill, J (2007) Strategies for preventing obesity. In: Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.

When I work prn in inpatient rehabilitation, I have access to each patient’s chart and can really focus on the systems review and past medical history, which often gives me ample reasons to ask about pelvic floor dysfunction. So, of course, I do. I have yet to find a gynecological cancer survivor who does not report an ongoing struggle with urinary incontinence. And sadly, they all report that they just deal with it.
Bretschneider et al.2016 researched the presence of pelvic floor disorders in females with presumed gynecological malignancy prior to surgical intervention. Baseline assessments were completed by 152 of the 186 women scheduled for surgery. The rate of urinary incontinence (UI) at baseline was 40.9% for the subjects, all of whom had uterine, ovarian, or cervical cancer. Stress urinary incontinence (SUI) was reported by 33.3% of the women, urge incontinence (UI) by 25%, fecal incontinence (FI) by 3.9%, abdominal pain by 47.4%, constipation by 37.7%, and diarrhea by 20.1%. The authors concluded pelvic floor disorders are prevalent among women with suspected gynecologic cancer and should be noted prior to surgery in order to provide more thorough rehabilitation for these women post-operatively.
Ramaseshan et al.2017 performed a systematic review of 31 articles to study pelvic floor disorder prevalence among women with gynecologic malignant cancers. Before treatment of cervical cancer, the prevalence of SUI was 24-29% (4-76% post-treatment), UI was 8-18% (4-59% post-treatment), and FI was 6% (2-34% post- treatment). Cervical cancer treatment also caused urinary retention (0.4-39%), fecal urge (3-49%), dyspareunia (12-58%), and vaginal dryness (15-47%). Uterine cancer showed a pre-treatment prevalence of SUI (29-36%), UUI (15-25%), and FI (3%) and post-treatment prevalence of UI (2-44%) and dyspareunia (7-39%). Vulvar cancer survivors had post-treatment prevalence of UI (4-32%), SUI (6-20%), and FI (1-20%). Ovarian cancer survivors had prevalence of SUI (32-42%), UUI (15-39%), prolapse (17%) and sexual dysfunction (62-75%). The authors concluded pelvic floor dysfunction is prevalent among gynecologic cancer survivors and needs to be addressed.
Lindgren, Dunberger, & Enblom2017 explored how gynecological cancer survivors (GCS) relate their incontinence to quality of life, view their physical activity/exercise ability, and perceive pelvic floor muscle training. The authors used a qualitative interview content analysis study with 13 women, age 48–82. Ten women had UI and 3 had FI after treatment (2 had radiation therapy, 5 had surgery, and 6 had surgery as well as radiation therapy). The results showed a reduction in physical and psychological quality of life and sexual activity because of incontinence. Having minimal to no experience or even awareness of pelvic floor training, 9 out of the 10 women were willing to spend 7 hours a week to improve their incontinence. Practical and emotional coping strategies also helped these women, and they all declared they had the cancer treatments without being informed of the risk of incontinence, which impacted their attitude and means of handling the situation.
Research shows incontinence is a common occurrence after gynecological cancer treatment. It impacts quality of life after surviving a serious illness, and many women do not know pelvic floor therapy can improve their situation. Oncology and the Female Pelvic Floor is an ideal course for practitioners to take to help increase their knowledge on how to educate and treat this population.
Bretschneider, C. E., Doll, K. M., Bensen, J. T., Gehrig, P. A., Wu, J. M., & Geller, E. J. (2016). Prevalence of pelvic floor disorders in women with suspected gynecological malignancy: a survey-based study. International Urogynecology Journal, 27(9), 1409–1414. http://doi.org/10.1007/s00192-016-2962-3
Ramaseshan, A.S., Felton, J., Roque, D., Rao, G., Shipper, A.G., Sanses, T.V.D. (2017). Pelvic floor disorders in women with gynecologic malignancies: a systematic review. International Urogynecology Journal. http://doi.org/10.1007/s00192-017-3467-4
Lindgren, A., Dunberger, G., & Enblom, A. (2017). Experiences of incontinence and pelvic floor muscle training after gynaecologic cancer treatment. Supportive Care in Cancer, 25(1), 157–166. http://doi.org/10.1007/s00520-016-3394-9
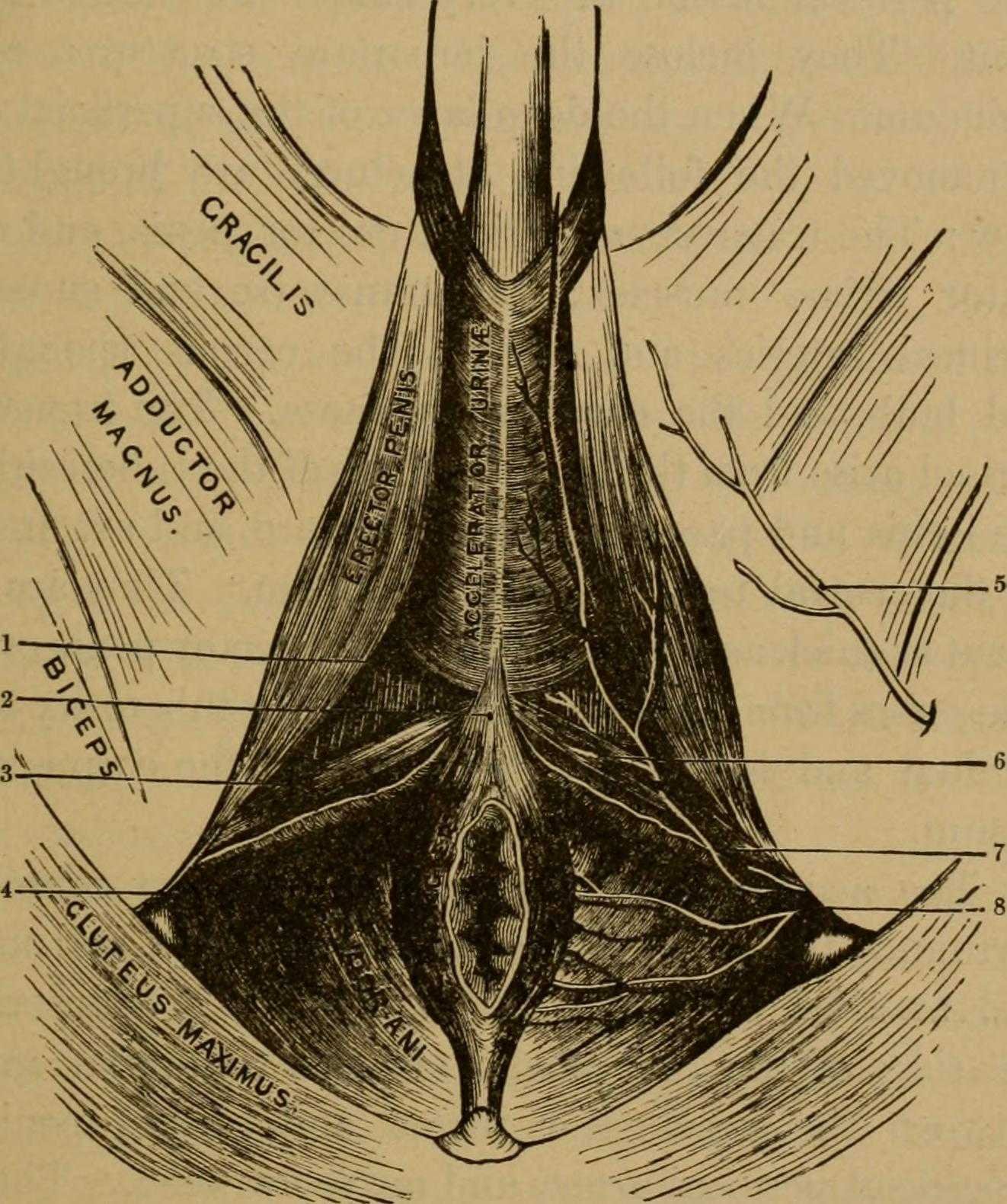
 Many therapists transition to treating men with the knowledge and training from female patients. When therapists apply this knowledge, for the most part, it works. When we spend some attention on learning what is a bit different, we might be drawn to the superficial muscles of the perineum. This old anatomy image does a wonderful job of "calling it like it is" or using anatomical terms that describe an action versus naming only the structure. In the image we are looking from below (inferior view) at the perineum and genitals. Just anterior to the anus we can see the anterior muscles within the urogenital triangle, with the base of the shaft of the penis located just anterior to (above in this image) the anus and perineal body. Notice that at the midline, we see muscle names the "accelerator urine". Modern textbooks refer to this muscle as the bulbocavernosus, or bulbospongiosus. Taking the name of accelerator urine, we can understand that this muscle will have an effect on aiding the body in emptying urine. It does this through rhythmic contractions, most often noted towards the end of urination, when the typical spurts of urine follow a more steady stream. This assistance with emptying can take place because the urethra is located within the lower part of the penis, the portion known as the corpus spongiosum. Because the bulbocavernosus muscle covers this part of the penis, and the inferior and lateral parts of the urethra are virtually wrapped within the bulbocavernosus, the muscle can have an effect on emptying the urine in the urethra.
Many therapists transition to treating men with the knowledge and training from female patients. When therapists apply this knowledge, for the most part, it works. When we spend some attention on learning what is a bit different, we might be drawn to the superficial muscles of the perineum. This old anatomy image does a wonderful job of "calling it like it is" or using anatomical terms that describe an action versus naming only the structure. In the image we are looking from below (inferior view) at the perineum and genitals. Just anterior to the anus we can see the anterior muscles within the urogenital triangle, with the base of the shaft of the penis located just anterior to (above in this image) the anus and perineal body. Notice that at the midline, we see muscle names the "accelerator urine". Modern textbooks refer to this muscle as the bulbocavernosus, or bulbospongiosus. Taking the name of accelerator urine, we can understand that this muscle will have an effect on aiding the body in emptying urine. It does this through rhythmic contractions, most often noted towards the end of urination, when the typical spurts of urine follow a more steady stream. This assistance with emptying can take place because the urethra is located within the lower part of the penis, the portion known as the corpus spongiosum. Because the bulbocavernosus muscle covers this part of the penis, and the inferior and lateral parts of the urethra are virtually wrapped within the bulbocavernosus, the muscle can have an effect on emptying the urine in the urethra.
Notice that if you follow the fibers of the accelerator urine muscle towards the top of the image, where the penis continues, you will notice fibers of the muscle wrapping around the sides of the penis. These fibers will continue as a fascial band that travels over the dorsal vessels of the penis. This allows the muscle to also have a significant action during sexual activity, in which blood flow (getting blood into, keeping blood in, and letting blood out of the penis) is paramount.
On either side of the penis we can see what is labeled the erector penis. As these muscles cover the legs, or crura which form the two upper parts of the penis, when the muscles contract, blood is shunted towards the main body of the penis. This of course helps with penile rigidity, as the smooth muscles in the artery walls of the penis allow blood to fill the spongy chambers.
Once we discuss the usual functions of these muscles, we can then imagine the dysfunctions potentially created by less than optimal activity. Consider the difficulty that these muscles will create in contracting or relaxing if they are either too weak, or too tense. These issues can create difficulty emptying well the urethra, often leading to post-void dribble. Blood flow and therefore penile rigidity with erections may be negatively impacted by inability of these muscles to contract or stay contracted, and blood flow leaving the penis may be impaired if the muscles cannot relax. When we work with patients who have genital pain, pelvic floor muscle weakness, dyscoordination, or tension, we can often improve sexual function, bladder emptying, and tasks that might otherwise be affected by pain.
If you are interested in learning more about how to assess and treat these muscles, you have one more opportunity this year to attend the 3-day Male Course instructed by Holly Tanner. Holly has been teaching this course for over 10 years when she co-wrote the first course with colleague and faculty member Stacey Futterman. The course has been updated and turned into a 3-day course to include more manual therapy techniques. Hurry to grab one of the remaining spots in the October 27-29 course in Grand Rapids!

At the peak of my racing career I won awards in all my races from 5k to marathon. While warming up I would scope out my competition, intimidated by muscular females wearing outfits to accentuate their physiques. Many times, appearance out-weighed running capacity. In a similar manner, one strong pelvic floor contraction produced by a female athlete does not always mean she has the endurance to stay dry in the long run.
 Brennand et al. (2017) researched urinary leakage during exercise in Canadian women. A summary of their findings concluded that skipping, trampoline, jumping jacks, and running/jogging were most likely to cause leakage. To combat the problem, 93.2% emptied their bladder just before exercise, 62.7% required voiding breaks during exercise, and 37.3% actually restricted their fluid intake to minimize leakage. While 90.3% of women who reported leakage impacted their activity just decreased their intensity, 80.7% avoided the activity entirely. Many women used pads (49.2%). Interest in pelvic floor physiotherapy to improve their UI was high (84.6%), but 63.5% of women still sought pessary or surgical management. Unfortunately, 35.6% of the women had no idea treatment was even an option.
Brennand et al. (2017) researched urinary leakage during exercise in Canadian women. A summary of their findings concluded that skipping, trampoline, jumping jacks, and running/jogging were most likely to cause leakage. To combat the problem, 93.2% emptied their bladder just before exercise, 62.7% required voiding breaks during exercise, and 37.3% actually restricted their fluid intake to minimize leakage. While 90.3% of women who reported leakage impacted their activity just decreased their intensity, 80.7% avoided the activity entirely. Many women used pads (49.2%). Interest in pelvic floor physiotherapy to improve their UI was high (84.6%), but 63.5% of women still sought pessary or surgical management. Unfortunately, 35.6% of the women had no idea treatment was even an option.
Nygaard & Shaw (2016) reviewed and summarized the cross-sectional studies regarding the association between physical activity and pelvic floor disorders. Trampolinists, especially those in the 3rd tertile of competition, even those who were nulliparous, experienced greater leakage. Competitive athletes in the highest quartile of time exercising were found to have 2.5 times the amount of urinary incontinence (UI) as the lowest inactive quartile; however, 2nd and 3rd quartile recreational athletes had no difference in UI compared to inactive women. Type and dosage of exercise were both factors in UI risk. Various studies showed habitual walking decreased UI in older women, moderate exercise decreased the risk of UI, and no exercise increased the risk of UI. The incidence of UI being related to having performed strenuous exercise early in life has been limited and variable, with one study of Norwegian athletes and US Olympians not having any greater UI later in life, while another showed middle-aged women who used to exercise 7.5 hours per week had a higher incidence of UI. This review also reported athletes had a 20% greater cross sectional area of the levator ani muscle and a greater pubovisceral muscle mean diameter; however, the pelvic floor strength recorded was lower than non-athletes.
Interestingly, Leitner et al. (2017) explored pelvic floor muscle activation for continent and incontinent females during running. For 10 seconds, EMG tripolar vaginal probe recorded activity at 7, 11, and 15km/h. No statistically significant differences between continent or incontinent subjects were found for the EMG values. Pre-activity and reflex activity mean EMG increased significantly with speed; mean pelvic floor muscle EMG activity during running was significantly above onset activation value; and, maximum voluntary contraction was exceeded 100% for all time intervals at 15km/h in women with UI. These authors suggested the stimulus of running could actually be beneficial in pelvic floor muscle training considering the reflex activity of the muscles.
At races now, I still silently survey my competition, but now I am more curious as to how many women are actually able to complete the run without leakage. The prevalence of UI among athletes continues and is becoming more of an open topic of conversation. The research as to how much and which kind of exercise correlates with UI or what activity and level of participation may be preventative for UI is growing. The need for pelvic floor therapists to treat athletes who are fit to be dry is ever increasing.
Brennand, E., Ruiz-Mirazo, E., Tang, S., Kim-Fine, S., Calgary Women’s Pelvic Health Research Group. (2017). Urinary leakage during exercise: problematic activities, adaptive behaviors, and interest in treatment for physically active Canadian women. International Urogynecology Journal. http://www.doi:10.1007/s00192-017-3409-1
Nygaard, I. E., & Shaw, J. M. (2016). Physical Activity and the Pelvic Floor. American Journal of Obstetrics and Gynecology, 214(2), 164–171. http://doi.org/10.1016/j.ajog.2015.08.067
Leitner M, Moser H, Eichelberger P, Kuhn A, Radlinger L. (2017). Evaluation of pelvic floor muscle activity during running in continent and incontinent women: An exploratory study. Neurourology and Urodynamics. 36:1570–1576. https://doi.org/10.1002/nau.23151

The first time I experienced the effects of Post-Traumatic Stress Disorder (PTSD) was when my patient dissociated during a treatment session and relived the rape that had occurred when she was ten years old. It was devastating. I didn’t know what to do. She was unresponsive to my intervention. Her eyes didn’t see me, alternating between wide-eyed, horrified panic and clenched-closed, lip biting excruciating pain. It was my late night and I was alone in the clinic. I sat helplessly next to my sweet patient hoping and praying that her torture would end quickly. When she finally stopped writhing, she slept. Deep and hard. Finally she woke up disoriented and scared. She grabbed her things and left. For me, this experience was my initiation into the world of trauma.
 Approximately 5-6 % of men and 10-12% of women will suffer from PTSD at some point in their lives. Researchers believe that 10% of people exposed to trauma will go on to develop PTSD. The expression of PTSD symptoms can present differently in men and women. Men may have more externalizing disorders progressing along a scale that includes vigilance, resistance, defiance, aggression and homicidal thoughts. Women tend to present with internalizing disorders such as depression, anxiety, exaggerated startle responses, dissociation, and suicidal thoughts. The research is clear that both men and women with PTSD display changes in brain function. The mid brain (amygdala, basal ganglia and hippocampus) tends to be overactive in sounding alarm signals while the prefrontal cortex fails to turn off the mid brain when a threat is no longer present. Since the prefrontal cortex is not always functioning correctly, traditional talk therapy may not be as effective for treating PTSD. Instead, say many researchers, breath and movement exercises may help regulate brain functioning. Yoga, Tai Chi, and meditation have been shown to have a positive impact on down regulating the mid brain and improving cerebral output. As pelvic floor therapists we deal with trauma on a daily basis, whether we know it or not. Although we are not trained in psychology, understanding PTSD and equipping ourselves with tools to support our patients is imperative for both our patients and ourselves.
Approximately 5-6 % of men and 10-12% of women will suffer from PTSD at some point in their lives. Researchers believe that 10% of people exposed to trauma will go on to develop PTSD. The expression of PTSD symptoms can present differently in men and women. Men may have more externalizing disorders progressing along a scale that includes vigilance, resistance, defiance, aggression and homicidal thoughts. Women tend to present with internalizing disorders such as depression, anxiety, exaggerated startle responses, dissociation, and suicidal thoughts. The research is clear that both men and women with PTSD display changes in brain function. The mid brain (amygdala, basal ganglia and hippocampus) tends to be overactive in sounding alarm signals while the prefrontal cortex fails to turn off the mid brain when a threat is no longer present. Since the prefrontal cortex is not always functioning correctly, traditional talk therapy may not be as effective for treating PTSD. Instead, say many researchers, breath and movement exercises may help regulate brain functioning. Yoga, Tai Chi, and meditation have been shown to have a positive impact on down regulating the mid brain and improving cerebral output. As pelvic floor therapists we deal with trauma on a daily basis, whether we know it or not. Although we are not trained in psychology, understanding PTSD and equipping ourselves with tools to support our patients is imperative for both our patients and ourselves.
You might be wondering what happened after that frightful night in the clinic? My patient was determined to get better. She had a non-relaxing pelvic floor. She was a teacher and was plagued by urinary distress. She either had terrible urgency or would go for hours and not be able to empty her bladder. So we met with her therapist to learn strategies to help us to be able to work together without triggering dissociation. It was a slow road, but the three of us working together helped my patient not only reach her goals but to be able to be skillful enough to maintain her gains using a dilator for self-treatment.
If you would like to learn more about PTSD, meditation, yoga, chronic pain, psychologically informed practice and self-care for patients and providers please join Nari Clemons and I in Tampa in January as we present a new offering for Herman and Wallace, “Holistic Intervention and Meditation.” We would love to see you there.
Bremner, J. D. (2006). Traumatic stress: effects on the brain. Dialogues in clinical neuroscience, 8(4), 445-461.
Kerr, C. E., Jones, S. R., Wan, Q., Pritchett, D. L., Wasserman, R. H., Wexler, A., ... & Littenberg, R. (2011). Effects of mindfulness meditation training on anticipatory alpha modulation in primary somatosensory cortex. Brain research bulletin, 85(3), 96-103.
Morasco, B. J., Lovejoy, T. I., Lu, M., Turk, D. C., Lewis, L., & Dobscha, S. K. (2013). The relationship between PTSD and chronic pain: mediating role of coping strategies and depression. Pain, 154(4), 609-616.
Olff, M., Langeland, W., & Gersons, B. P. (2005). The psychobiology of PTSD: coping with trauma. Psychoneuroendocrinology, 30(10), 974-982.
The Role Of Yoga In Healing Trauma

While running on my treadmill, I watched a commercial advertising specially designed pads as “the solution” for women athletes who “leak” during their sport. Before my introduction to Herman and Wallace Rehabilitation Institute, I would have rushed to the nearest store to buy a case of them. When we don’t know how to fix a problem, we tend to cling to bandages to cover them, allowing us to ignore them. With 29 years of running and racing and 2 natural childbirths under my belt, leaks have happened, and it is common. However, leaks due to urinary stress incontinence are not normal and do not stop simply because you place a contoured, sporty, sanitary pad in the lining of your shorts.
 A 2016 cross-sectional study by Ameida et al. investigated urinary incontinence (UI) and pelvic floor dysfunctions (PFD) such as constipation, anal incontinence, pelvic organ prolapse, vaginal laxity, and dyspareunia in female athletes who participate in high-impact sports. The 67 amateur athletes and 96 non-athletes completed an ad hoc survey to determine PFD symptoms. Artistic gymnasts, trampolinists, swimmers, and judo participants were among the athletes with the highest risk of urinary incontinence. Although the athletes had a higher risk of UI, they reported less constipation, less straining to relieve themselves, and less manual assistance for defecation than the non-athletes. The authors were able to conclude that high impact sports or sports requiring a strong effort put athletes at risk for UI, uncontrolled gas expulsion, and even sexual dysfunction. They emphasize a need for attention to be given to pelvic floor training for rehabilitation as well as preventative strategies and education for high risk yet asymptomatic athletes.
A 2016 cross-sectional study by Ameida et al. investigated urinary incontinence (UI) and pelvic floor dysfunctions (PFD) such as constipation, anal incontinence, pelvic organ prolapse, vaginal laxity, and dyspareunia in female athletes who participate in high-impact sports. The 67 amateur athletes and 96 non-athletes completed an ad hoc survey to determine PFD symptoms. Artistic gymnasts, trampolinists, swimmers, and judo participants were among the athletes with the highest risk of urinary incontinence. Although the athletes had a higher risk of UI, they reported less constipation, less straining to relieve themselves, and less manual assistance for defecation than the non-athletes. The authors were able to conclude that high impact sports or sports requiring a strong effort put athletes at risk for UI, uncontrolled gas expulsion, and even sexual dysfunction. They emphasize a need for attention to be given to pelvic floor training for rehabilitation as well as preventative strategies and education for high risk yet asymptomatic athletes.
In 2015, DaRoza et al. performed a cross-sectional cohort study to determine the urinary leakage in 22 young female trampolinists based on the volume of their training and level of ranking. Leakage was assessed by the International Consultation on Incontinence Questionnaire Short-Form (ICIQ-UI-SF), and another questionnaire determined each athlete’s championship ranking and training volume. An astounding 72.7% of girls reported urine leakage since starting to perform on the trampoline, and the greatest severity was significantly associated with the highest training volume. The impact of UI on the athlete’s quality of life was greatest in this 3rd tertile. The authors recommended these athletes with a high frequency of UI be educated on the impact of their sport on their pelvic floor muscles and proposed they get treated by pelvic health professionals to minimize or resolve the incontinence.
Thankfully, none of the above researchers or medical professionals advises the study participants to just use a pad and carry on with their sport. Urinary incontinence is a real problem in athletes, and its prevalence is appalling. Even young girls without any birthing of babies to blame are leaking. Making females (and males) aware of the impact sports can have on their pelvic floor and educating them that urinary leakage is not normal are essential missions for healthcare professionals. “The Athlete and the Pelvic Floor” course can help integrate pivotal aspects of pelvic rehabilitation into sports medicine, as some conditions just may require training to move down to the pelvic floor for complete recovery.
Almeida, MB, Barra, AA, Saltiel, F, Silva-Filho, AL, Fonseca, AM, Figueiredo, EM. (2016). Urinary incontinence and other pelvic floor dysfunctions in female athletes in Brazil: A cross-sectional study. Scandinavian Journal of Medicine & Science in Sports. 26(9):1109-16. http://doi:10.1111/sms.12546
Da Roza, T, Brandão, S, Mascarenhas, T, Jorge, RN, Duarte JA. (2015). Volume of training and the ranking level are associated with the leakage of urine in young female trampolinists. Clinical Journal of Sport Medicine. 25(3):270-5. http://DOI:10.1097/JSM.0000000000000129
The Center for Disease Control reports that prostate cancer is the most common form of male cancer in the United States (just ahead of lung cancer and colorectal cancer), and the American Cancer Society estimates that 1 in 7 men will be diagnosed with prostate cancer at some point in their lifetime. With prostate cancer being so common, it is likely that a male with symptoms of urinary incontinence following a prostatectomy may show up at your clinic’s door for treatment. What do you do? Whether you have extensive training for male pelvic floor disorders or are just starting your initial training for pelvic floor dysfunctions, you likely have some intervention skills to help this population.
A recent case report in the Journal of Women’s Health Physical Therapy, outlines management of a 76-year-old male patient with mixed urinary incontinence postprostatectomy 10 years. This case report does a nice job describing not just physical therapy (PT) interventions, but also multifaceted management of a typical patient post radical prostatectomy. The case report describes a thorough history, systems review, pelvic floor muscle (PFM) examination, tests &measures, and outcome assessment. Our discussion will focus on interventions as you may already possess the skills for several of the treatments included in this patient’s plan of care.
The patient’s complaints were mixed urinary incontinence (UI) symptoms including 3-4 pads per day and 1 pad at night. He reported nocturia 3-4 times per night. 2-3 times per week he had large UI episodes that soaked his outwear. Also, he complained of inability to delay voiding, and UI with walking to the bathroom, sit to stand, lifting, coughing, and sneezing.
For the patients’ urge UI symptoms, behavioral interventions were utilized. The patient completed PFM contractions to inhibit detrusor contractions and suppress urgency (urge control technique). Educating the patient on correct PFM contraction isolation was a very important component of this patients’ treatment. Verbal, digital, and surface electromyography (sEMG) techniques were used to ensure correct PFM contraction and to reduce Valsalva. Clinical decision making for home exercise program utilized dominant PFM fiber types and the patients’ performance on the PERFECT PFM strength testing system described by Laycock. (External Urethral Sphincter is predominantly Type II fast twitch muscle fiber in males and Levator Ani is predominantly Type I slow twitch.) For the home program, the patient completed progressive reps and sets of 10” (targets slow twitch) and 2” (targets fast twitch) PFM isometrics in supine progressing to standing. (There is a chart with additional details on PFM home program for each visit in the case report.) Additionally, instruct and use of “the knack” (volitional PFM contraction before and during cough or other physical exertions to prevent UI) for activities that the patient usually had UI with including sit to stand transfer, lifting, coughing, and sneezing was essential for the patients’ symptoms. PFM coordination training with sEMG helped reduce his accessory muscle recruitment patterns and Valsalva. Bladder retraining and lifestyle recommendation were important (per his 3-day bladder diary) as he was consuming 3 cups of coffee and 4 cups or more of tea a day, likely contributing to urgency and urge UI symptoms. Also, he was informed regarding the effect of obesity on UI (as his BMI was 35.9 placing him in the obese range) and that modest amounts of weight loss maybe sufficient for UI reduction. Abdominal exercises targeting Transversus Abdominus were also prescribed for their role in core support with PFM’s. Lastly, electrical stimulation was not included in this patients’ plan of care due to the patients’ cardiac history and pacemaker, as well as, he could initiate PFM contraction and utilize urge control techniques appropriately.
The outcome for this patient was positive. He attended 5 PT sessions over a 3-month period. He did have to cancel two appointments between the 4th and 5th visits due to an emergency surgery to place two cardiac stents. He had reduced urinary leakage indicated by reduced undergarment changes and reduced pad usage per day. His pads were less saturated and he no longer had leakage that spread to his outwear. He had a 50% reduction in UI episodes reported on his bladder diary and a 50% reduction in nocturia from 4 times to 2 times per night. He reported reduced daily urinary frequency from 7 to 5 times per day with no instances of severe urgency. He demonstrated improved PERFECT score of 4, 10, 8, 10 (initially his score was 2, 5, 3, 5) indicating improved PFM strength and endurance. Also, he had improved PFM coordination as he could isolate PFM contraction without Valsalva or accessory muscle activation. He also had one strength grade improvement with abdominal strength. All that being said, most importantly, this patient had improved rating on the outcome questionnaire (International Continence Society male Short Form (ICSmaleSF)) at discharge indicating improved quality of life. At initial evaluation, this patient rated “a lot” (3 on ICSmaleSF) when asked how much the urinary symptoms interfered with his life, at discharge he reported “not at all” (0 on ICSmaleSF).
One component to this case that I found fascinating was the duration of time that had passed since this patients’ prostatectomy. It had been 10 years since this patient had his surgical procedures. He had never been offered physical therapy or knew about it as a possible treatment for his symptoms. Additionally, that he could have such success with improvements in voiding and incontinence function, as well as improved quality of life as long as 10 years’ post-prostatectomy.
This case report is a comprehensive glimpse of what physical therapy assessment and treatment may look like for a patient with urinary dysfunction following radical prostatectomy. This patient had great improvements with positive changes enhancing his quality of life. So, if you are considering adding treatment of this population to your practice consider attending Post-Prostatectomy Patient Rehabilitation, available this July in Annapolis, MD or September in Seattle, WA.
"Cancer Among Men", Centers for Disease Control and Prevention
Roscow, A. S., & Borello-France, D. (2016). Treatment of Male Urinary Incontinence Post–Radical Prostatectomy Using Physical Therapy Interventions. Journal of Women’s Health Physical Therapy, 40(3), 129-138.

An 80 year old lady who had seen a physical therapist where I once worked in Naperville, IL, just completed a marathon and a 5k race in one weekend. She is undoubtedly one woman who can change our perception of the “elderly,” but we all know her strength and ability are not the norm. The geriatric patients coming to therapy for pelvic floor disorders are more likely to be too frail to have run a mile this century, and they are most likely struggling with functional ADLs, as research suggests.
 A study by Erekson et al., (2015) looked into the prevalence of frailty, cognitive impairment, and functional disability among women over 65 years of age looking for the best treatment for their pelvic floor dysfunction (PFD). A major concern was the presence of frailty being equated with poorer surgical outcomes. The 150 women in the study were tested with the Fried Frailty Index to measure frailty, the Saint Louis University Mental Status Score for cognitive screening, and the Katz ADL score for functional status. Pelvic organ prolapse was present in 65.3% women, urinary incontinence in 20.7%, overactive bladder in 9.3%, and anal incontinence in 0.7%. Sixteen percent of women were considered frail and 42% were “prefrail.” Dementia was determined in 21.3% of women, and functional disability in 30.7%. Pelvic floor dysfunction in women with frailty caused a significantly greater life-impact than in normal and pre-frail women. Forty-six percent of the subjects opted for surgery, but only women with functional disability, not impaired cognition nor frailty, were less likely to choose non-surgical intervention. The authors concluded that being able to identify women with PFD with risk factors of frailty, cognitive impairment, and functional disability may help predict the risk of complications before surgery and help encourage behavioral changes and provide the appropriate pre and post-operative care for each woman.
A study by Erekson et al., (2015) looked into the prevalence of frailty, cognitive impairment, and functional disability among women over 65 years of age looking for the best treatment for their pelvic floor dysfunction (PFD). A major concern was the presence of frailty being equated with poorer surgical outcomes. The 150 women in the study were tested with the Fried Frailty Index to measure frailty, the Saint Louis University Mental Status Score for cognitive screening, and the Katz ADL score for functional status. Pelvic organ prolapse was present in 65.3% women, urinary incontinence in 20.7%, overactive bladder in 9.3%, and anal incontinence in 0.7%. Sixteen percent of women were considered frail and 42% were “prefrail.” Dementia was determined in 21.3% of women, and functional disability in 30.7%. Pelvic floor dysfunction in women with frailty caused a significantly greater life-impact than in normal and pre-frail women. Forty-six percent of the subjects opted for surgery, but only women with functional disability, not impaired cognition nor frailty, were less likely to choose non-surgical intervention. The authors concluded that being able to identify women with PFD with risk factors of frailty, cognitive impairment, and functional disability may help predict the risk of complications before surgery and help encourage behavioral changes and provide the appropriate pre and post-operative care for each woman.
Silay et al., (2016) published a review on urinary incontinence (UI) in elderly women, relating its association with other geriatric conditions. Sixty-four females aged 65 and older were evaluated using the Turkish version of the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) to assess UI and quality of life. Activities of daily living (ADL) and instrumental activities of daily living (IADL) were used to evaluate functional status, and the Mini Mental State Examination was used for cognitive assessment. The comorbidities, pharmaceuticals, falls, and body mass index (BMI) of patients were also recorded. Results showed the subjects’ rate of urinary incontinence was 40.6%, and 28.1% of the women had their quality of life impacted. There was a statistically significant association using logistic regression between UI and quality of life, functional status, and comorbidity. Sadly, 50% of patients thought UI was normal with aging, 34.6% had been embarrassed to tell anyone about it, and 15.3% said they did not know UI was something for which medical treatment could be given.
Understanding how to manage frailty, cognitive issues, and functional deficits of our elderly patients can positively impact treatment outcomes. We should always strive to educate our patients and be aware of conditions that may be affecting or even contributing to their PFD. The Geriatric Pelvic Floor Rehab course can enlighten therapists on a score of comorbidities and techniques for handling those patients who are not sporting a marathon finisher medal to their physical therapy visits!
Erekson, E. A., Fried, T. R., Martin, D. K., Rutherford, T. J., Strohbehn, K., & Bynum, J. P. W. (2015). Frailty, cognitive impairment, and functional disability in older women with female pelvic floor dysfunction. International Urogynecology Journal, 26(6), 823–830. http://doi.org/10.1007/s00192-014-2596-2
K. Silay, S. Akinci, A. Ulas, A. Yalcin, Y.S. Silay, M.B. Akinci, I. Dilek, B. Yalcin. (2016). Occult urinary incontinence in elderly women and its association with geriatric condition. European Review for Medical and Pharmacological Sciences. 20(3): 447-451.

When my 6 year old daughter ran to the bathroom 3-4 times before she got on the school bus every morning, I wasn’t too concerned, but I definitely took note. The day she was in tears and wouldn’t get off the toilet because she felt like she was still wet, I got worried (although slightly intrigued). No matter how much she wiped, she still felt wet. When she stood up, she felt like she was going to pee herself, making my sweet-natured girl slip into hysterics. After eliminating small amounts of urine 8 separate times in 3 hours and saying it burned, I assumed she had a urinary tract infection (UTI). A simple urine test ruled out UTI or diabetes (thankfully!). So then, what was my daughter’s diagnosis? The pediatrician simply referred to it as “a phase;” however, I had researched the symptoms before the visit.
 In 2014 Arlen et al. described a condition called “phantom urinary incontinence.” This refers to the situation when children experience the sensation of being wet (a presumptive urinary incontinence) when they are objectively dry. They considered 20 children (18 females, 2 males) referred to their pediatric urology clinic over a 5 year span, all who were all diagnosed with phantom urinary incontinence (PUI). The authors evaluated the concomitant diagnoses found among the boys and girls in the study. Lower urinary tract symptoms were present in 95% of the subjects. Associated bladder symptoms were found as well, with urgency in 75% and frequency in 50% of the children. Vaginitis occurred in 72% of the girls. Parents reported obsessive-compulsive disorder or obsessive-compulsive disorder personality traits in 70% of the children. In order to treat these patients, dietary modifications, timed voiding, and a bowel regimen were implemented to manage symptoms. A follow up at 14.4 months revealed 90% of the children’s bowel-bladder dysfunction improved and PUI resolved. The authors concluded children compliant with a rigid bladder-bowel regimen experience relief of their “phantom” incontinence as well as lower urinary tract symptoms, and a majority of PUI patients have obsessive-compulsive traits.
In 2014 Arlen et al. described a condition called “phantom urinary incontinence.” This refers to the situation when children experience the sensation of being wet (a presumptive urinary incontinence) when they are objectively dry. They considered 20 children (18 females, 2 males) referred to their pediatric urology clinic over a 5 year span, all who were all diagnosed with phantom urinary incontinence (PUI). The authors evaluated the concomitant diagnoses found among the boys and girls in the study. Lower urinary tract symptoms were present in 95% of the subjects. Associated bladder symptoms were found as well, with urgency in 75% and frequency in 50% of the children. Vaginitis occurred in 72% of the girls. Parents reported obsessive-compulsive disorder or obsessive-compulsive disorder personality traits in 70% of the children. In order to treat these patients, dietary modifications, timed voiding, and a bowel regimen were implemented to manage symptoms. A follow up at 14.4 months revealed 90% of the children’s bowel-bladder dysfunction improved and PUI resolved. The authors concluded children compliant with a rigid bladder-bowel regimen experience relief of their “phantom” incontinence as well as lower urinary tract symptoms, and a majority of PUI patients have obsessive-compulsive traits.
Oliver et al., (2013) studied how psychosocial comorbidities and body mass index relate to children with lower urinary tract dysfunction. Data on 358 patients with lower urinary tract dysfunction between 6 to 17 years old was collected, and the subjects’ parents completed questionnaires screening for lower urinary tract symptoms, stressful life events, and psychological comorbidities. Obesity was present in 28.5% of the children, 22.9% had a recent stress in life, and 22.9% had a psychiatric disorder. Under and overweight children, children with a recent life stressor, psychiatric disorder, or both, as well as the younger-aged children all had lower urinary tract symptom scores significantly higher than healthy weight subjects, those without psychosocial comorbidities, and older subjects. The results encourage screening for psychosocial issues and obesity in pediatric patients with lower urinary tract dysfunction.
Having read the research, I knew a life stressor was likely contributing to my daughter’s symptoms. I had already advised her to sit on the toilet every 1-2 hours, don’t let her bladder get too full, wipe gently from front to back, stop bubble baths, and wear looser pants. To conclude our $76 session, the doctor prescribed almost verbatim what my daughter had heard from me at home. Although thankful it wasn’t something more serious, I am curious what the diagnosis code is for “a phase” and when it will end.
Arlen, AM, Dewhurst, LL, Kirsch, SS, Dingle, AD, Scherz, HC, Kirsch, AJ. (2014). Phantom urinary incontinence in children with bladder-bowel dysfunction. Urology. 84(3):685-8. DOI: http://dx.doi.org/10.1016/j.urology.2014.04.046 Oliver, J.L., Campigotto, M.J., Coplen, D.E. et al,. (2013). Psychosocial comorbidities and obesity are associated with lower urinary tract symptoms in children with voiding dysfunction. The Journal of Urology. 190:1511–1515. DOI: http://dx.doi.org/10.1016/j.juro.2013.02.025

When I bring up the topic of pelvic floor dysfunction in athletes, stress urinary incontinence (SUI) is usually the first aspect of pelvic health that springs to mind – and rightly so, as professional sport is one of the risk factors for stress urinary incontinence Poswiata et al 2014. The majority of studies show that the average prevalence of urinary incontinence across all sports is 50%, with SUI being the most common lower urinary tract symptom. Athletes are constantly subject to repeated sudden & considerable rises in intra-abdominal pressure: e.g. heel striking, jumping, landing, dismounting and racquet loading.
What’s less often discussed is the topic of gastrointestinal dysfunction in athletes. Anal incontinence in athletes is not well documented, although a study from Vitton et al in 2011 found a higher prevalence than in age matched controls (conversely a study by Bo & Braekken in 2007 found no incidence). More recently, Nygaard reported earlier this year (2016) that young women participating in high-intensity activity are more likely to report anal incontinence than less active women.
A presentation by Colleen Fitzgerald, MD at the American Urogynecologic Society meeting in 2014 highlighted the multifaceted nature of pelvic floor dysfunction in female athletes, specifically in this case, triathletes. The study found that one in three female triathletes suffers from a pelvic floor disorder such as urinary incontinence, bowel incontinence and pelvic organ prolapse. One in four had one component of the "female athlete triad", a condition characterized by decreased energy, menstrual irregularities and abnormal bone density from excessive exercise and inadequate nutrition. Researchers surveyed 311 women for this study with a median age range of 35 – 44. These women were involved with triathlete groups and most (82 percent) were training for a triathlon at the time of the survey. On average, survey participants ran 3.7 days a week, biked 2.9 days a week and swam 2.4 days a week.
Of those who reported pelvic floor disorder symptoms, 16% had urgency urinary incontinence, 37.4% had stress urinary incontinence, 28% had bowel incontinence and 5% had pelvic organ prolapse. Training mileage and intensity were not associated with pelvic floor disorder symptoms. 22% of those surveyed screened positive for disordered eating, 24% had menstrual irregularities and 29% demonstrated abnormal bone strength. With direct access becoming a reality for many of us, we must acknowledge the need for specific questioning when it comes to pelvic health issues, as well as the ability to recognise signs and symptoms of the female athlete triad in our patients.
Want to learn more about pelvic health for athletes? Join me in beautiful Arlington this November 5-6 at The Athlete and the Pelvic Floor!
J Hum Kinet. 2014 Dec 9; 44: 91–96 Published online 2014 Dec 30. doi:10.2478/hukin-2014-0114 PMCID: PMC4327384. Prevalence of Stress Urinary Incontinence in Elite Female Endurance Athlete Anna Poświata, Teresa Socha and Józef Opara1
J Womens Health (Larchmt). 2011 May;20(5):757-63. doi: 10.1089/jwh.2010.2454. Epub 2011 Apr 18. Impact of high-level sport practice on anal incontinence in a healthy young female population. Vitton V, Baumstarck-Barrau K, Brardjanian S, Caballe I, Bouvier M, Grimaud JC.
Am J Obstet Gynecol. 2016 Feb;214(2):164-71. doi: 10.1016/j.ajog.2015.08.067. Epub 2015 Sep 6. Physical activity and the pelvic floor. Nygaard IE, Shaw JM.
All Upcoming Continuing Education Courses



Pelvic Function Level 1 - Satellite - Des Moines IA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Minneapolis MN - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Paso Robles CA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - St. Augustine FL - July 26 - 27 2025
Jul 26 2025 - Jul 27 2025

Pelvic Function Level 1 - Satellite - Virginia Beach VA - July 26 - 27 2025 - SOLD OUT
Jul 26 2025 - Jul 27 2025


Pelvic Function Level 1 - In-Person - Chicago IL - August 2 - 3 2025 - SOLD OUT
Aug 2 2025 - Aug 3 2025



Menopause Transitions and Pelvic Rehab - Remote Course - August 9 - 10 2025
Aug 9 2025 - Aug 10 2025










Pelvic Function Level 2C - Satellite - Palm Beach FL - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025

Pelvic Function Level 2C - Satellite - New Orleans LA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025
Pelvic Function Level 2C - Satellite - Paso Robles CA - August 16 - 17 2025
Aug 16 2025 - Aug 17 2025



Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Jacksonville FL - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Pelvic Function Level 1 - Satellite - Chicago IL - August 23 - 24 2025 - SOLD OUT
Aug 23 2025 - Aug 24 2025


Pelvic Function Level 1 - Satellite - Hermosa Beach CA - August 23 - 24 2025
Aug 23 2025 - Aug 24 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Indianapolis IN - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Indianapolis IN - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Rehabilitative Ultrasound Imaging: Women's Health - Satellite Lab Course - Seattle WA - September 5 - 7 2025
Sep 5 2025 - Sep 7 2025
Rehabilitative Ultrasound Imaging: Orthopedic Topics Satellite Lab Course - Seattle WA - September 5 - 6 2025
Sep 5 2025 - Sep 6 2025

Pelvic Function Level 1 - Satellite - Sacramento CA - September 6 - 7 2025 - SOLD OUT
Sep 6 2025 - Sep 7 2025


Pelvic Function Level 1 - Satellite - San Francisco CA - September 6 - 7 2025 - SOLD OUT
Sep 6 2025 - Sep 7 2025